Division of Child Neurology, Lucile Packard Children's Hospital at Stanford University, Dr Levy 750 Welch Road Suite 317, Palo Alto, CA, USA.
Division of Medical Genetics, Lucile Packard Children's Hospital at Stanford University, Palo Alto, CA, USA.
Neurocrit Care. 2022 Feb;36(1):30-38. doi: 10.1007/s12028-021-01313-1. Epub 2021 Jul 28.
Guidelines recommend evaluation for electrographic seizures in neonates and children at risk, including after cardiopulmonary bypass (CPB). Although initial research using screening electroencephalograms (EEGs) in infants after CPB found a 21% seizure incidence, more recent work reports seizure incidences ranging 3-12%. Deep hypothermic cardiac arrest was associated with increased seizure risk in prior reports but is uncommon at our institution and less widely used in contemporary practice. This study seeks to establish the incidence of seizures among infants following CPB in the absence of deep hypothermic cardiac arrest and to identify additional risk factors for seizures via a prediction model.
A retrospective chart review was completed of all consecutive infants ≤ 3 months who received screening EEG following CPB at a single center within a 2-year period during 2017-2019. Clinical and laboratory data were collected from the perioperative period. A prediction model for seizure risk was fit using a random forest algorithm, and receiver operator characteristics were assessed to classify predictions. Fisher's exact test and the logrank test were used to evaluate associations between clinical outcomes and EEG seizures.
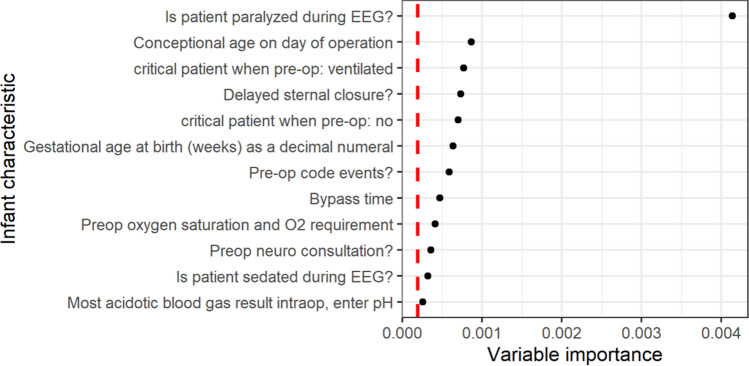
A total of 112 infants were included. Seizure incidence was 10.7%. Median time to first seizure was 28.1 h (interquartile range 18.9-32.2 h). The most important factors in predicting seizure risk from the random forest analysis included postoperative neuromuscular blockade, prematurity, delayed sternal closure, bypass time, and critical illness preoperatively. When variables captured during the EEG recording were included, abnormal postoperative neuroimaging and peak lactate were also highly predictive. Overall model accuracy was 90.2%; accounting for class imbalance, the model had excellent sensitivity and specificity (1.00 and 0.89, respectively).
Seizure incidence was similar to recent estimates even in the absence of deep hypothermic cardiac arrest. By employing random forest analysis, we were able to identify novel risk factors for postoperative seizure in this population and generate a robust model of seizure risk. Further work to validate our model in an external population is needed.
指南建议对电癫痫发作进行评估,包括新生儿和有风险的儿童,包括体外循环(CPB)后。尽管最初的研究使用 CPB 后婴儿的筛查脑电图(EEG)发现癫痫发作发生率为 21%,但最近的研究报告癫痫发作发生率为 3-12%。在之前的报告中,深低温心脏停搏与癫痫发作风险增加相关,但在我们的机构中并不常见,在当代实践中也较少使用。本研究旨在确定无深低温心脏停搏的 CPB 后婴儿癫痫发作的发生率,并通过预测模型确定其他癫痫发作的危险因素。
对 2017 年至 2019 年期间在单一中心接受 CPB 后接受筛查脑电图的所有连续婴儿(≤3 个月)进行回顾性图表审查。收集围手术期的临床和实验室数据。使用随机森林算法拟合癫痫发作风险预测模型,并评估接收者操作特征以分类预测。Fisher 精确检验和对数秩检验用于评估临床结果与 EEG 癫痫发作之间的关联。
共纳入 112 例婴儿。癫痫发作发生率为 10.7%。首次癫痫发作的中位时间为 28.1 小时(四分位距 18.9-32.2 小时)。随机森林分析中预测癫痫发作风险最重要的因素包括术后神经肌肉阻滞、早产、延迟胸骨闭合、体外循环时间和术前危重病。当包括脑电图记录期间捕获的变量时,异常术后神经影像学和峰值乳酸也具有高度预测性。总体模型准确性为 90.2%;考虑到类别不平衡,该模型具有出色的敏感性和特异性(分别为 1.00 和 0.89)。
即使没有深低温心脏停搏,癫痫发作的发生率也与最近的估计相似。通过采用随机森林分析,我们能够确定该人群术后癫痫发作的新危险因素,并生成癫痫发作风险的强大模型。需要进一步的工作来在外部人群中验证我们的模型。