School of Cancer Sciences, Faculty of Medicine, University of Southampton, Southampton, United Kingdom.
F. Hoffmann-La Roche Ltd, Basel, Switzerland.
Blood Adv. 2021 Aug 10;5(15):2935-2944. doi: 10.1182/bloodadvances.2020003985.
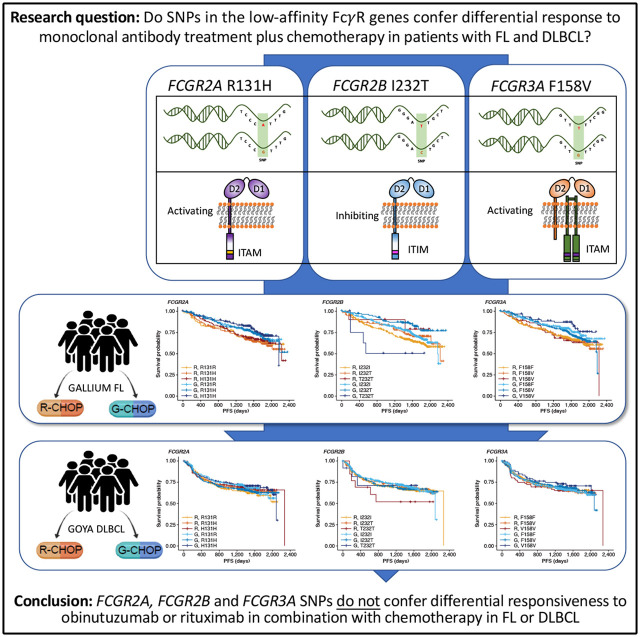
Single-nucleotide polymorphisms (SNPs) have been shown to influence Fcγ receptor (FcγR) affinity and activity, but their effect on treatment response is unclear. We assessed their importance in the efficacy of obinutuzumab or rituximab combined with chemotherapy in untreated advanced follicular lymphoma (FL) and diffuse large B-cell lymphoma (DLBCL) in the GALLIUM (www.clinicaltrials.gov #NCT01332968) and GOYA (#NCT01287741) trials, respectively. Genomic DNA was extracted from patients enrolled in GALLIUM (n = 1202) and GOYA (n = 1418). Key germline SNPs, FCGR2A R131H (rs1801274), FCGR3A F158V (rs396991), and FCGR2B I232T (rs1050501), were genotyped and assessed for their impact on investigator-assessed progression-free survival (PFS). In both cohorts there was no prognostic effect of FCGR2A or FCGR3A. In FL, FCGR2B was associated with favorable PFS in univariate and multivariate analyses comparing I232T with I232I, with a more modest association for rituximab-treated (univariate: hazard ratio [HR], 0.78; 95% confidence interval [CI], 0.54-1.14; P = .21) vs obinutuzumab-treated patients (HR, 0.56; 95% CI, 0.34-0.91; P = .02). Comparing T232T with I232I, an association was found for obinutuzumab (univariate: HR, 2.76; 95% CI, 1.02-7.5; P = .0459). Neither observation retained significance after multiple-test adjustment. FCGR2B was associated with poorer PFS in multivariate analyses comparing T232T with I232I in rituximab- but not obinutuzumab-treated patients with DLBCL (HR, 4.40; 95% CI, 1.71-11.32; P = .002; multiple-test-adjusted P = .03); however, this genotype was rare (n = 13). This study shows that FcγR genotype is not associated with response to rituximab/obinutuzumab plus chemotherapy in treatment-naive patients with advanced FL or DLBCL.
单核苷酸多态性(SNPs)已被证明会影响 Fcγ 受体(FcγR)的亲和力和活性,但它们对治疗反应的影响尚不清楚。我们评估了它们在未经治疗的晚期滤泡性淋巴瘤(FL)和弥漫性大 B 细胞淋巴瘤(DLBCL)中,奥滨尤妥珠单抗或利妥昔单抗联合化疗的疗效中的重要性,分别在 GALLIUM(www.clinicaltrials.gov #NCT01332968)和 GOYA(#NCT01287741)试验中进行了研究。从 GALLIUM(n = 1202)和 GOYA(n = 1418)入组的患者中提取基因组 DNA。对关键的种系 SNPs,FcγR2A R131H(rs1801274)、FcγR3A F158V(rs396991)和 FcγR2B I232T(rs1050501)进行基因分型,并评估其对研究者评估的无进展生存期(PFS)的影响。在两个队列中,FcγR2A 或 FcγR3A 均无预后作用。在 FL 中,FcγR2B 与 I232T 与 I232I 的单变量和多变量分析中的有利 PFS 相关,而与利妥昔单抗治疗的患者(单变量:风险比[HR],0.78;95%置信区间[CI],0.54-1.14;P =.21)相比,与奥滨尤妥珠单抗治疗的患者(HR,0.56;95%CI,0.34-0.91;P =.02)的相关性更为温和。与 I232I 相比,T232T 在奥滨尤妥珠单抗治疗的患者中存在相关性(单变量:HR,2.76;95%CI,1.02-7.5;P =.0459)。在多变量分析中,比较 T232T 与 I232I,在利妥昔单抗治疗的患者中,FcγR2B 与较差的 PFS 相关,但在奥滨尤妥珠单抗治疗的患者中则不相关(HR,4.40;95%CI,1.71-11.32;P =.002;多重检验调整后的 P =.03);然而,这种基因型很少见(n = 13)。本研究表明,在未经治疗的晚期 FL 或 DLBCL 患者中,FcγR 基因型与利妥昔单抗/奥滨尤妥珠单抗联合化疗的反应无关。