Vercoulen Timon F G, Doodkorte Remco J P, Roth Alex, de Bie Rob, Willems Paul C
Department of Orthopaedic Surgery, Research School CAPHRI, Maastricht University Medical Center, Maastricht, The Netherlands.
Department of Epidemiology, Research School CAPHRI, Maastricht University Medical Center, Maastricht, The Netherlands.
Global Spine J. 2022 Jul;12(6):1282-1296. doi: 10.1177/21925682211034500. Epub 2021 Jul 30.
Systematic review.
To summarize the results of clinical studies investigating spinal instrumentation techniques aiming to reduce the postoperative incidence of proximal junctional kyphosis (PJK) and/or failure (PJF) in adult spinal deformity (ASD) patients.
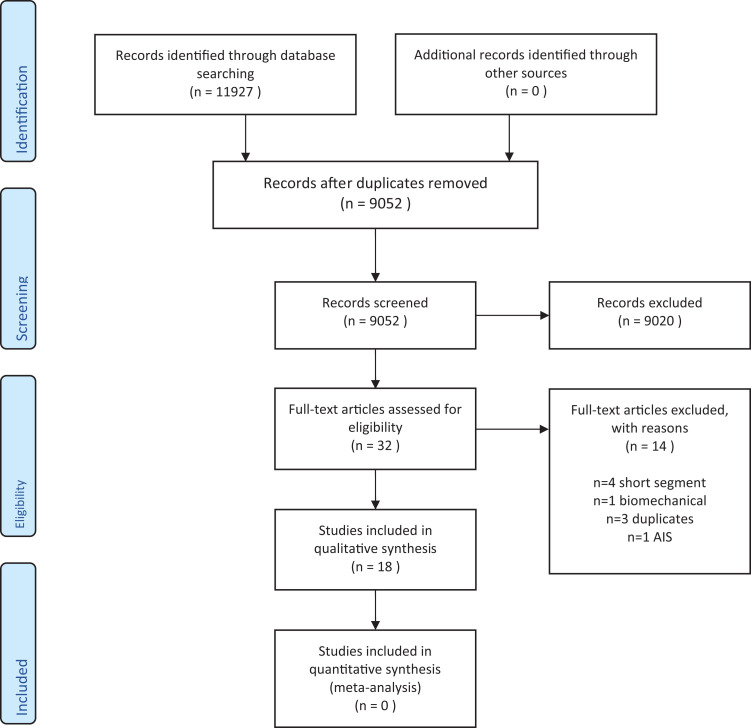
EMBASE and Medline® were searched for articles dating from January 2000 onward. Data was extracted by 2 independent authors and methodological quality was assessed using ROBINS-I.
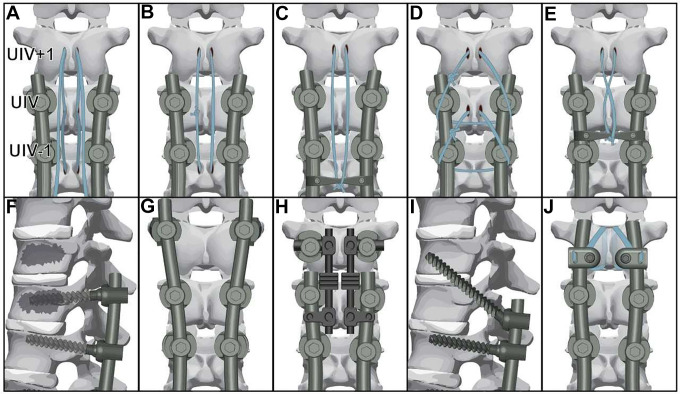
18 retrospective- and prospective cohort studies with a severe or critical risk of bias were included. Different techniques were applied at the upper instrumented vertebra (UIV): tethers in various configurations, 2-level prophylactic vertebroplasty (2-PVP), transverse process hooks (TPH), flexible rods (FR), sublaminar tapes (ST) and multilevel stabilization screws (MLSS). Compared to a pedicle screw (PS) group, significant differences in PJK incidence were found using tethers in various configurations (18% versus 45%, = 0.001, 15% versus 38%, = 0.045), 2-PVP (24% vs 36%, = 0.020), TPH (0% vs. 30%, = 0.023) and FR (15% versus 38%, = 0.045). Differences in revision rates for PJK were found in studies concerning tethers (4% versus 18%, = 0.002), 2-PVP (0% vs 13%, = 0.031) and TPH (0% vs 7%, = n.a.).
Although the studies are of low quality, the most frequently studied techniques, namely 2-PVP as anterior reinforcement and (tensioned) tethers or TPH as posterior semi-rigid fixation, show promising results. To provide a reliable comparison, more controlled studies need to be performed, including the use of clinical outcome measures and a uniform definition of PJF.
系统评价。
总结旨在降低成人脊柱畸形(ASD)患者近端交界性后凸(PJK)和/或失败(PJF)术后发生率的脊柱内固定技术的临床研究结果。
检索EMBASE和Medline®中2000年1月起的文章。由2名独立作者提取数据,并使用ROBINS - I评估方法学质量。
纳入18项存在严重或关键偏倚风险的回顾性和前瞻性队列研究。在上固定椎(UIV)应用了不同技术:各种构型的束带、两级预防性椎体成形术(2 - PVP)、横突钩(TPH)、柔性棒(FR)、椎板下带(ST)和多级稳定螺钉(MLSS)。与椎弓根螺钉(PS)组相比,使用各种构型束带(18%对45%,P = 0.001;15%对38%,P = 0.045)、2 - PVP(24%对36%,P = 0.020)、TPH(0%对30%,P = 0.023)和FR(15%对38%,P = 0.045)时,PJK发生率存在显著差异。在关于束带(4%对18%,P = 0.002)、2 - PVP(0%对13%,P = 0.031)和TPH(0%对7%,P = 无数据)的研究中发现了PJK翻修率的差异。
尽管这些研究质量较低,但研究最频繁的技术,即作为前路加强的2 - PVP和作为后路半刚性固定的(张紧的)束带或TPH,显示出有前景的结果。为了进行可靠的比较,需要开展更多对照研究,包括使用临床结局指标和对PJF进行统一界定。