Quantitative Pharmacology Department, EMD Serono Research and Development Institute, 45A Middlesex Turnpike, Billerica, MA, 01821, USA.
Merck Institute for Pharmacometrics (an affiliate of Merck KGaA, Darmstadt, Germany), Lausanne, Switzerland.
Eur J Drug Metab Pharmacokinet. 2021 Sep;46(5):601-611. doi: 10.1007/s13318-021-00706-z. Epub 2021 Jul 30.
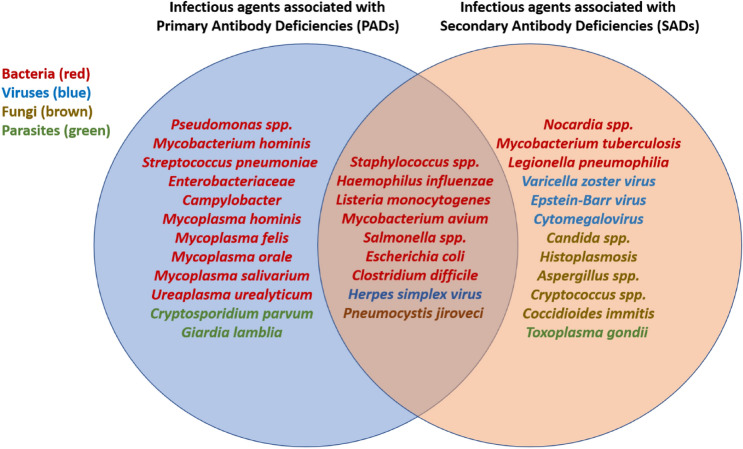
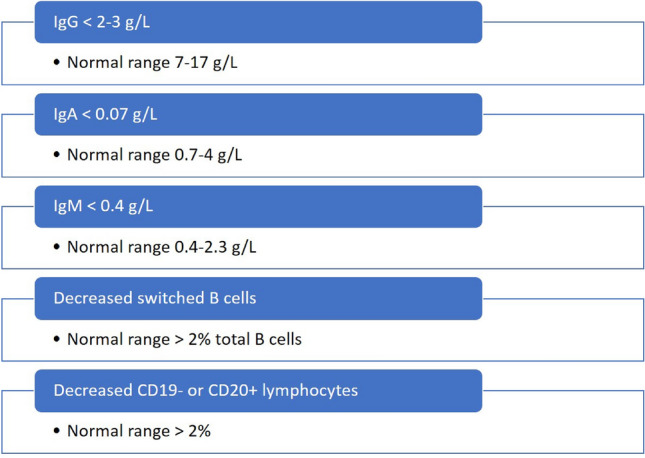
Immunosuppressive drugs can alleviate debilitating symptoms of autoimmune diseases, but, by the same token, excessive immune suppression can result in an increased risk of infection. Despite the dangers of a compromised immune system, clear definitions of what constitutes excessive suppression remain elusive. Here we review the most common infections associated with primary antibody deficiencies (PADs), such as agammaglobulinemia, common variable immunodeficiency (CVID), and IgA deficiency, as well as infections that are associated with drug-induced or secondary antibody immunodeficiencies (SADs). We identify a number of bacterial, viral, and fungal infections (e.g., Listeria monocytogenes, Staphylococcus sp., Salmonella spp., Escherichia coli, influenza, varicella zoster virus, and herpes simplex virus) associated with both PADs and SADs, and suggest that diagnostic criteria for PADs could be used as a first-line measure to identify potentially unsafe levels of immune suppression in SADs. Specifically, we suggest that, based on PAD diagnostic criteria, IgG levels should remain above 2-3 g/L, IgA levels should not fall below 0.07 g/L, and IgM levels should remain above 0.4 g/L to prevent immunosuppressive drugs from inducing mimicking PAD-like effects. We suggest that these criteria could be used in the early stages of drug development, and that pharmacokinetic and pharmacodynamic modeling could help guide patient selection to potentially improve drug safety. We illustrate the proposed approach using atacicept as an example and conclude with a discussion of the applicability of this approach for other drugs that may induce excessive immune suppression.
免疫抑制药物可以缓解自身免疫性疾病的衰弱症状,但同样地,过度的免疫抑制会增加感染的风险。尽管免疫系统受损存在风险,但明确界定过度抑制的标准仍然难以捉摸。在这里,我们回顾了与原发性抗体缺陷(PAD)相关的最常见感染,如丙种球蛋白缺乏症、常见可变免疫缺陷(CVID)和 IgA 缺乏症,以及与药物诱导或继发性抗体免疫缺陷(SAD)相关的感染。我们确定了一些与 PAD 和 SAD 相关的细菌、病毒和真菌感染(例如李斯特菌、葡萄球菌、沙门氏菌、大肠杆菌、流感、水痘带状疱疹病毒和单纯疱疹病毒),并建议将 PAD 的诊断标准用作识别 SAD 中潜在不安全免疫抑制水平的一线措施。具体来说,我们建议,根据 PAD 的诊断标准,IgG 水平应保持在 2-3g/L 以上,IgA 水平不应低于 0.07g/L,IgM 水平应保持在 0.4g/L 以上,以防止免疫抑制药物引起类似 PAD 的效应。我们建议在药物开发的早期阶段使用这些标准,并且药代动力学和药效学模型可以帮助指导患者选择,从而有可能提高药物安全性。我们使用阿替西普作为一个例子来说明所提出的方法,并讨论了该方法对可能引起过度免疫抑制的其他药物的适用性。