GeoHealth Group, Institute of Global Health, University of Geneva, Geneva, Switzerland.
Institute for Environmental Sciences, University of Geneva, Geneva, Switzerland.
BMJ Open. 2021 Jul 30;11(7):e045891. doi: 10.1136/bmjopen-2020-045891.
Improving access to emergency obstetrical and neonatal care (EmONC) is a key strategy for reducing maternal and neonatal mortality. Access is shaped by several factors, including service availability and geographical accessibility. In 2013, the Ministry of Health (MoH) of Togo used service availability and other criteria to designate particular facilities as EmONC facilities, facilitating efficient allocation of limited resources. In 2018, the MoH further revised and rationalised this health facility network by applying an innovative methodology using health facility characteristics and geographical accessibility modelling to optimise timely access to EmONC services. This study compares the geographical accessibility of the network established in 2013 and the smaller network developed in 2018.
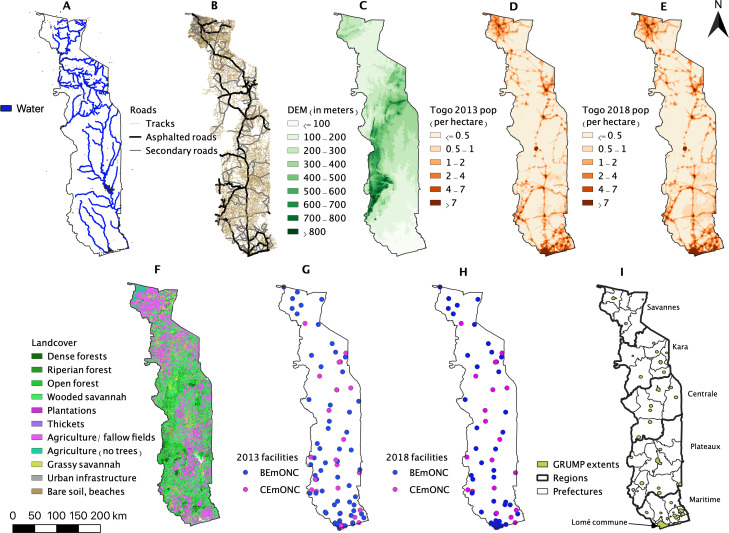
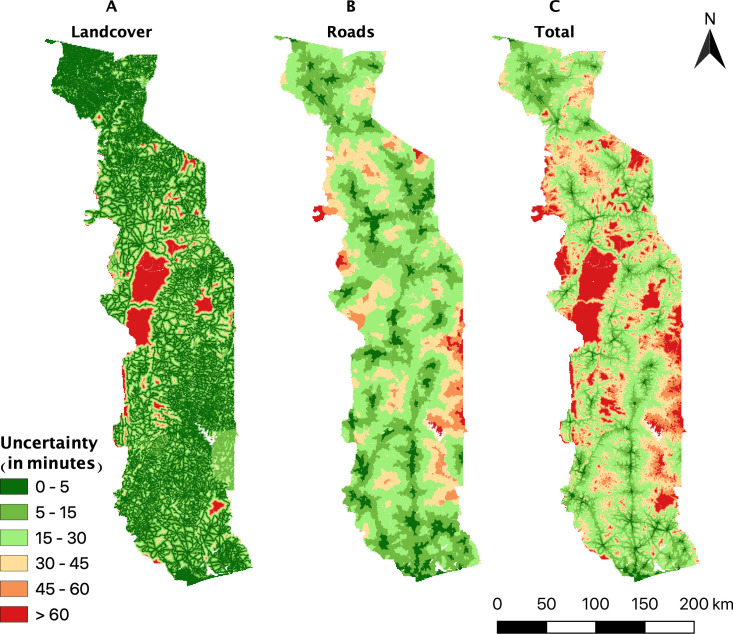
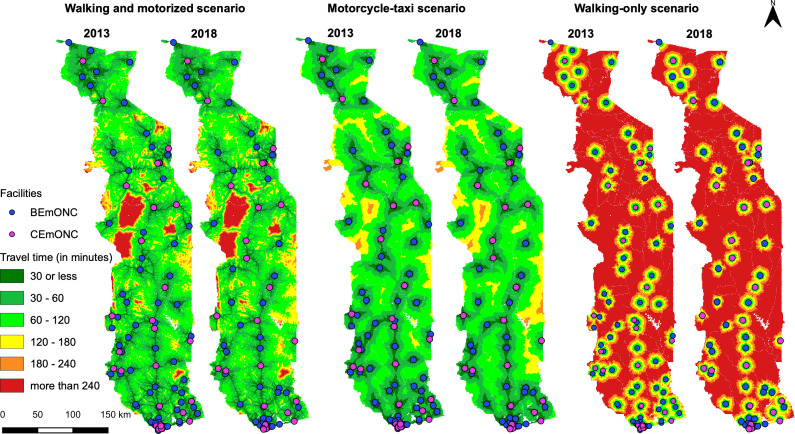
We used data regarding travel modes and speeds, geographical barriers and topographical and urban constraints, to estimate travel times to the nearest EmONC facilities. We compared the EmONC network of 109 facilities established in 2013 with the one composed of 73 facilities established in 2018, using three travel scenarios (walking and motorised, motorcycle-taxi and walking-only).
When walking and motorised travel is considered, the 2013 EmONC network covers 81% and 96.6% of the population at the 1-hour and 2-hour limit, respectively. These figures are slightly higher when motorcycle-taxis are considered (82.8% and 98%), and decreased to 34.7% and 52.3% for the walking-only scenario. The 2018 prioritised EmONC network covers 78.3% (1-hour) and 95.5% (2-hour) of the population for the walking and motorised scenario.
By factoring in geographical accessibility modelling to our iterative EmONC prioritisation process, the MoH was able to decrease the designated number of EmONC facilities in Togo by about 30%, while still ensuring that a high proportion of the population has timely access to these services. However, the physical access to EmONC for women unable to afford motorised transport remains inequitable.
改善紧急产科和新生儿护理(EmONC)的可及性是降低孕产妇和新生儿死亡率的关键策略。可及性受到服务可用性和地理可及性等因素的影响。2013 年,多哥卫生部(MoH)利用服务可用性和其他标准指定了特定的设施作为 EmONC 设施,以有效地分配有限的资源。2018 年,MoH 进一步修订和合理化了这个卫生设施网络,采用了一种创新的方法,利用卫生设施的特点和地理可及性建模来优化及时获得 EmONC 服务的机会。本研究比较了 2013 年建立的网络和 2018 年发展的较小网络的地理可及性。
我们使用有关旅行方式和速度、地理障碍以及地形和城市限制的数据来估计到最近的 EmONC 设施的旅行时间。我们比较了 2013 年建立的 109 个设施的 EmONC 网络和 2018 年建立的 73 个设施的网络,使用了三种旅行情景(步行和机动、摩托车出租车和仅步行)。
当考虑步行和机动旅行时,2013 年的 EmONC 网络在 1 小时和 2 小时的限制内分别覆盖了 81%和 96.6%的人口。当考虑使用摩托车出租车时,这一数字略有上升(分别为 82.8%和 98%),而在仅步行的情况下则下降到 34.7%和 52.3%。2018 年的优先 EmONC 网络在步行和机动情景下分别覆盖了 78.3%(1 小时)和 95.5%(2 小时)的人口。
通过在我们的迭代 EmONC 优先排序过程中纳入地理可及性建模,MoH 能够将多哥指定的 EmONC 设施数量减少约 30%,同时仍然确保大多数人口能够及时获得这些服务。然而,无法负担机动交通的妇女获得 EmONC 的实际途径仍然是不平等的。