Zhou Xiaoyang, Pan Weihao, Chen Bixin, Xu Zhaojun, Pan Jianneng
Department of Intensive Care Medicine, HwaMei Hospital, University of Chinese Academy of Sciences, Ningbo, 315000, Zhejiang, China.
Ningbo Institute of Life and Health Industry, University of Chinese Academy of Sciences, Ningbo, 315000, Zhejiang, China.
Ann Intensive Care. 2021 Jul 31;11(1):119. doi: 10.1186/s13613-021-00909-2.
Dynamic arterial elastance (Ea) has been extensively considered as a functional parameter of arterial load. However, conflicting evidence has been obtained on the ability of Ea to predict mean arterial pressure (MAP) changes after fluid expansion. This meta-analysis sought to assess the predictive performance of Ea for the MAP response to fluid expansion in mechanically ventilated hypotensive patients.
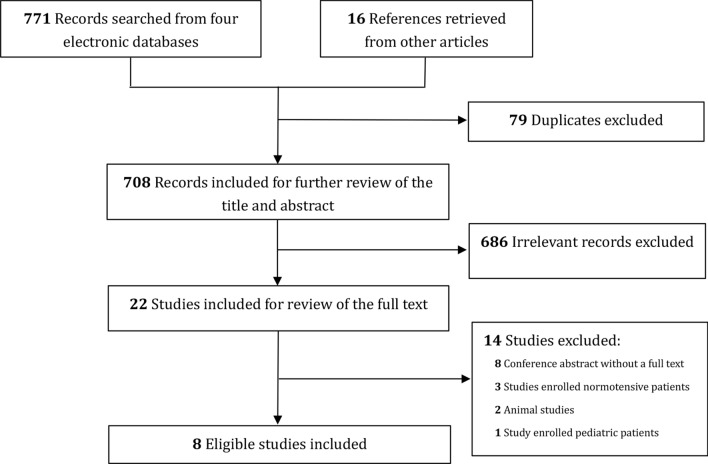
We systematically searched electronic databases through November 28, 2020, to retrieve studies that evaluated the association between Ea and fluid expansion-induced MAP increases in mechanically ventilated hypotensive adults. Given the diverse threshold value of Ea among the studies, we only reported the area under the hierarchical summary receiver operating characteristic curve (AUHSROC) as the primary measure of diagnostic accuracy.
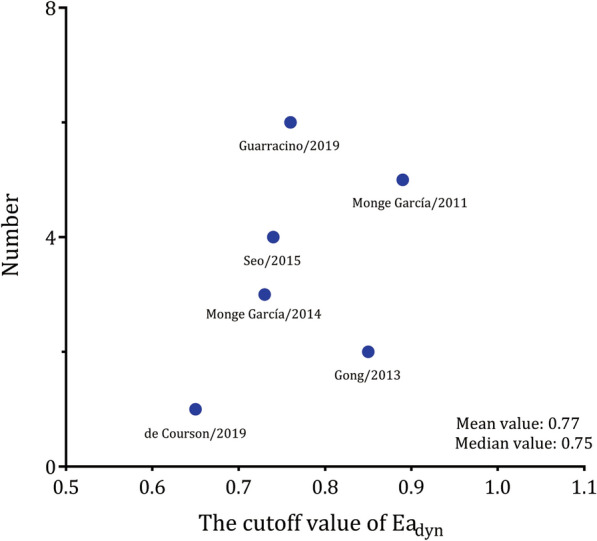
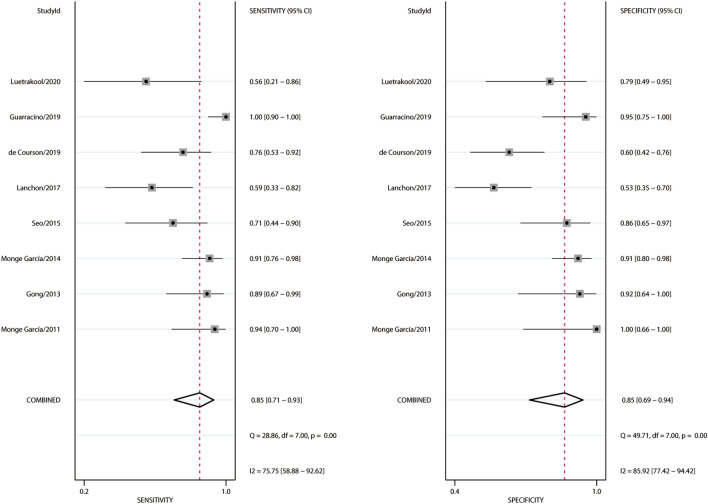
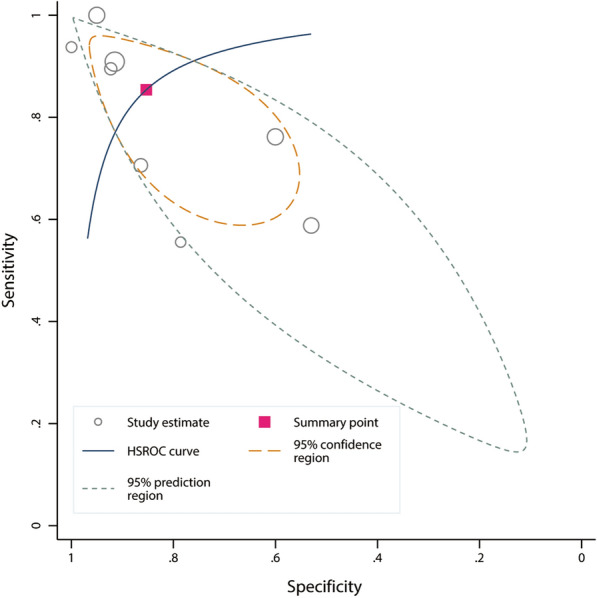
Eight observational studies that included 323 patients with 361 fluid expansions met the eligibility criteria. The results showed that Ea was a good predictor of MAP increases in response to fluid expansion, with an AUHSROC of 0.92 [95% confidence interval (CI) 0.89 to 0.94]. Six studies reported the cut-off value of Ea, which ranged from 0.65 to 0.89. The cut-off value of Ea was nearly conically symmetrical, most data were centred between 0.7 and 0.8, and the mean and median values were 0.77 and 0.75, respectively. The subgroup analyses indicated that the AUHSROC was slightly higher in the intensive care unit (ICU) patients (0.96; 95% CI 0.94 to 0.98) but lower in the surgical patients in the operating room (0.72; 95% CI 0.67 to 0.75). The results indicated that the fluid type and measurement technique might not affect the diagnostic accuracy of Ea. Moreover, the AUHSROC for the sensitivity analysis of prospective studies was comparable to that in the primary analysis.
Ea exhibits good performance for predicting MAP increases in response to fluid expansion in mechanically ventilated hypotensive adults, especially in the ICU setting.
动态动脉弹性(Ea)已被广泛视为动脉负荷的一个功能参数。然而,关于Ea预测液体扩容后平均动脉压(MAP)变化能力的证据存在矛盾。这项荟萃分析旨在评估Ea对机械通气的低血压患者液体扩容后MAP反应的预测性能。
我们系统检索了截至2020年11月28日的电子数据库,以检索评估Ea与机械通气的低血压成年患者液体扩容引起的MAP升高之间关联的研究。鉴于各研究中Ea的阈值不同,我们仅报告分层汇总接受者操作特征曲线下面积(AUHSROC)作为诊断准确性的主要指标。
八项观察性研究纳入了323例患者的361次液体扩容情况,符合纳入标准。结果显示,Ea是液体扩容后MAP升高的良好预测指标,AUHSROC为0.92[95%置信区间(CI)0.89至0.94]。六项研究报告了Ea的截断值,范围为0.65至0.89。Ea的截断值几乎呈圆锥对称,大多数数据集中在0.7至0.8之间,平均值和中位数分别为0.77和0.75。亚组分析表明,重症监护病房(ICU)患者的AUHSROC略高(0.96;95%CI 0.94至0.98),而手术室的外科患者则较低(0.72;95%CI 0.67至0.75)。结果表明,液体类型和测量技术可能不会影响Ea的诊断准确性。此外,前瞻性研究敏感性分析的AUHSROC与初步分析中的相当。
Ea在预测机械通气的低血压成年患者液体扩容后MAP升高方面表现良好,尤其是在ICU环境中。