Department of Anesthesia and Critical Care Medicine, Azienda Ospedaliero Universitaria Pisana, Pisa, Italy.
Department of Critical Care Medicine, University of Pittsburgh, 1215.4 Kaufmann Medical Building, 3471 Fifth Avenue, Pittsburgh, PA, 15213, USA.
Crit Care. 2019 Apr 15;23(1):118. doi: 10.1186/s13054-019-2414-9.
We hypothesized that the cardiovascular responses to Surviving Sepsis Guidelines (SSG)-defined resuscitation are predictable based on the cardiovascular state.
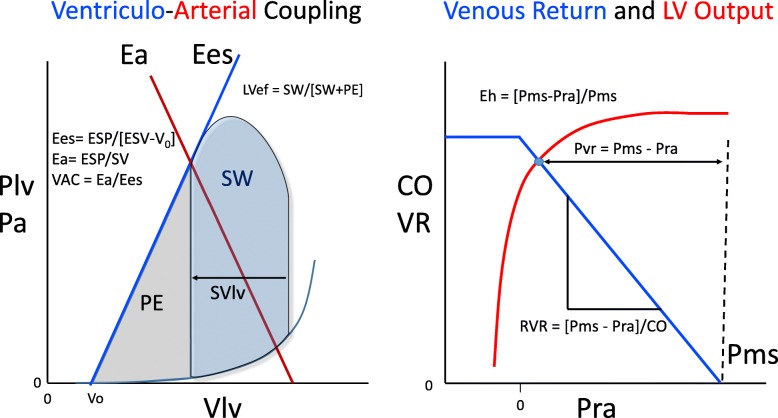
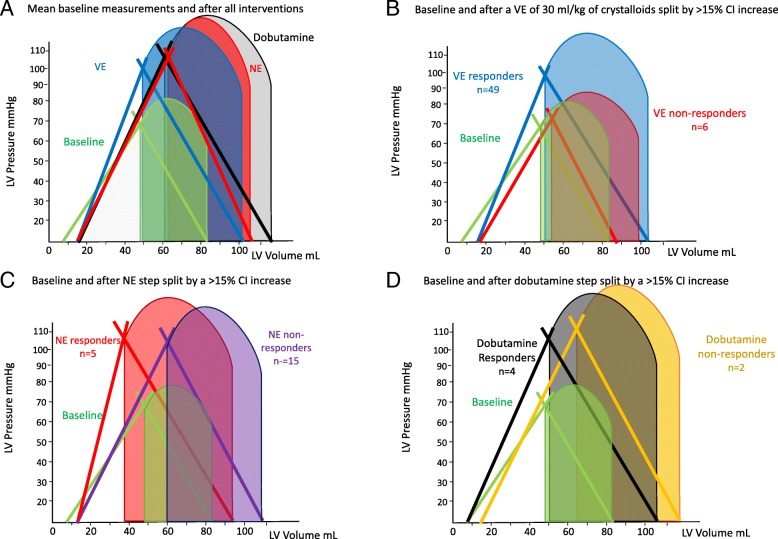
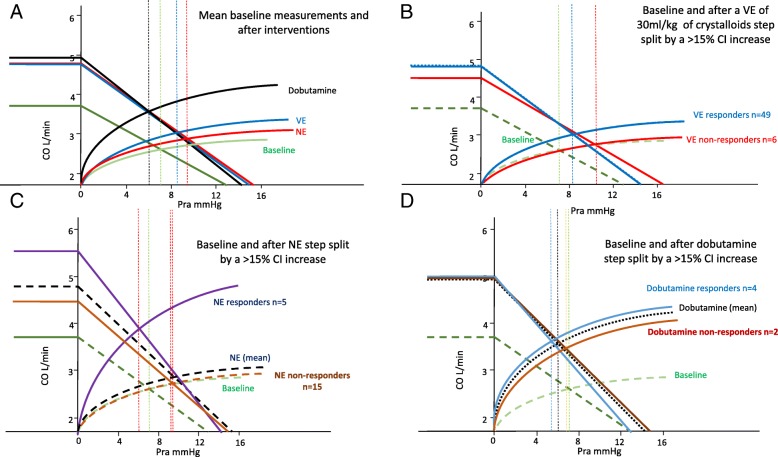
Fifty-five septic patients treated by SSG were studied before and after volume expansion (VE), and if needed norepinephrine (NE) and dobutamine. We measured mean arterial pressure (MAP), cardiac index (CI), and right atrial pressure (Pra) and calculated pulse pressure and stroke volume variation (PPV and SVV), dynamic arterial elastance (Ea), arterial elastance (Ea) and left ventricular (LV) end-systolic elastance (Ees), Ees/Ea (VAC), LV ejection efficiency (LVeff), mean systemic pressure analogue (Pmsa), venous return pressure gradient (Pvr), and cardiac performance (Eh), using standard formulae.
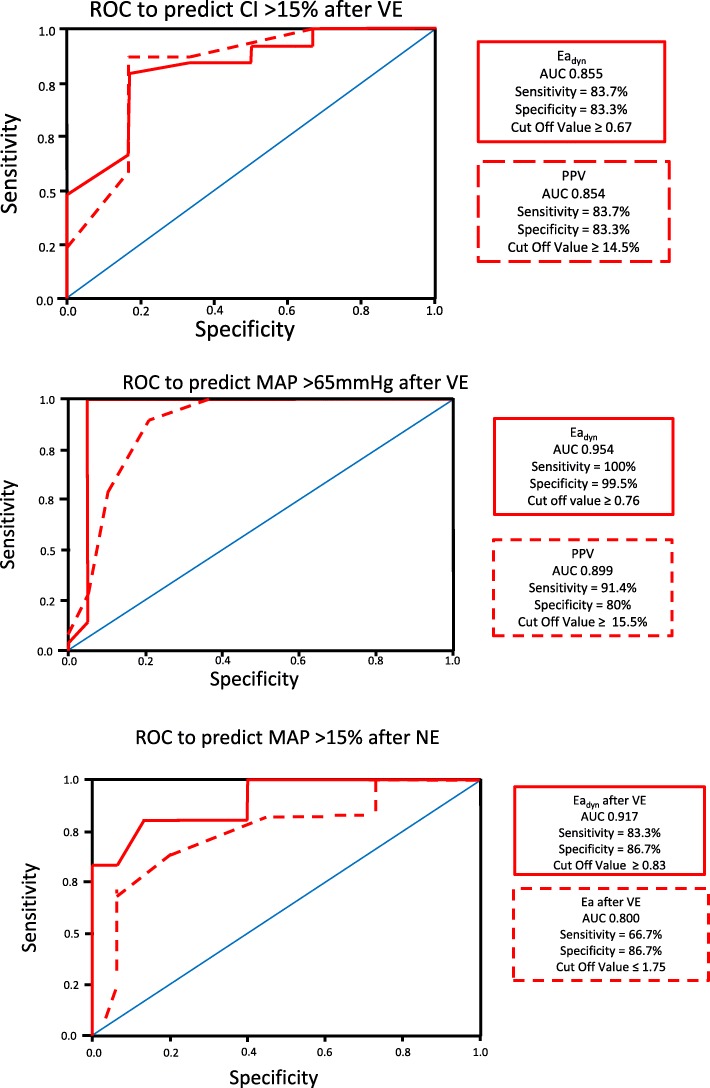
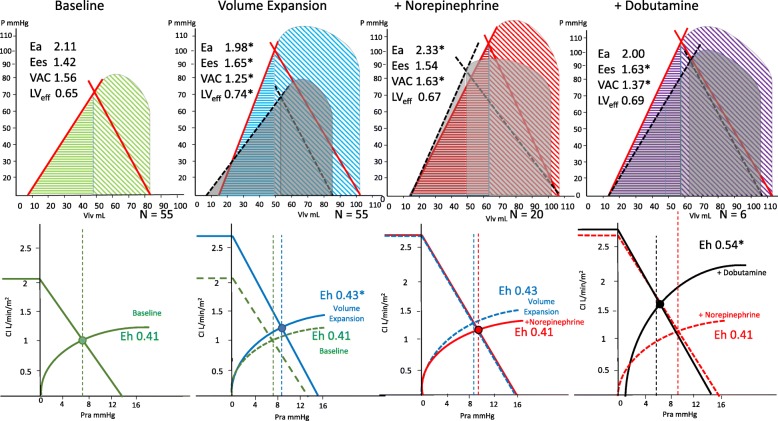
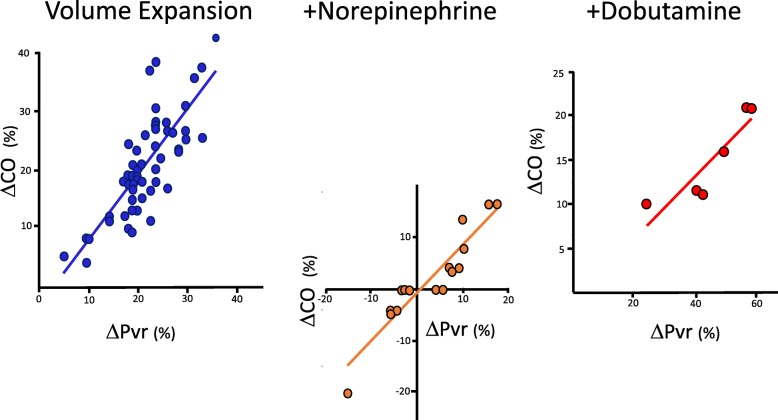
All patients were hypotensive (MAP 56.8 ± 3.1 mmHg) and tachycardic (113.1 ± 7.5 beat min), with increased lactate levels (lactate = 5.0 ± 4.2 mmol L) with a worsened VAC. CI was variable but > 2 L min M in 74%. Twenty-eight-day mortality was 48% and associated with admission lactate, blood urea nitrogen (BUN), and creatinine levels but not cardiovascular state. In all patients, both MAP and CI improved following VE, as well as cardiac contractility (Ees). Fluid administration improved Pra, Pmsa, and Pvr in all patients, whereas both HR and Ea decreased after VE, thus normalizing VAC. CI increases were proportional to baseline PPV and SVV. CI increases proportionally decreased PPV and SVV. VE increased MAP > 65 mmHg in 35/55 patients. MAP responders had higher PPV, SVV, and Ea than non-responders. NE was given to 20/55 patients in septic shock, but increased MAP > 65 mmHg in only 12. NE increased Ea, Ea, Pra, Pmsa, and VAC while decreasing HR, PPV, SVV, and LVeff. MAP responders had higher pre-NE Ees and lower VAC. Dobutamine was given to 6/8 patients who remained hypotensive following NE. It increased Ees, MAP, CI, and LVeff, while decreasing HR, Pra, and VAC. At all times and all steps of the protocol, CI changes were proportional to Pvr changes independent of treatment.
The cardiovascular response to SSG-based resuscitation is highly heterogeneous but predictable from pre-treatment measures of cardiovascular state.
我们假设,根据心血管状态,可预测对脓毒症指南(SSG)定义的复苏的心血管反应。
对 55 例接受 SSG 治疗的脓毒症患者进行研究,在容量复苏(VE)前后,以及需要时给予去甲肾上腺素(NE)和多巴酚丁胺。我们测量平均动脉压(MAP)、心指数(CI)和右心房压(Pra),并计算脉压和每搏量变异(PPV 和 SVV)、动脉弹性(Ea)、左心室(LV)收缩末期弹性(Ees)、Ees/Ea(VAC)、LV 射血效率(LVeff)、平均系统压力模拟(Pmsa)、静脉回流压力梯度(Pvr)和心脏性能(Eh),使用标准公式。
所有患者均出现低血压(MAP 56.8 ± 3.1mmHg)和心动过速(113.1 ± 7.5 次/分),伴有乳酸水平升高(乳酸= 5.0 ± 4.2mmol/L),VAC 恶化。CI 变化不定,但 74%的患者>2L/min/M。28 天死亡率为 48%,与入院时的乳酸、血尿素氮(BUN)和肌酐水平有关,但与心血管状态无关。在所有患者中,VE 后 MAP 和 CI 均改善,Ees 也改善。在所有患者中,液体输入均改善了 Pra、Pmsa 和 Pvr,而 VE 后 HR 和 Ea 均降低,从而使 VAC 正常化。CI 增加与基础 PPV 和 SVV 成正比。CI 增加与 PPV 和 SVV 呈比例降低。VE 使 35/55 名患者的 MAP 增加>65mmHg。MAP 反应者的 PPV、SVV 和 Ea 均高于无反应者。20/55 例脓毒性休克患者给予 NE,但只有 12 例 MAP 增加>65mmHg。NE 增加了 Ea、Ea、Pra、Pmsa 和 VAC,同时降低了 HR、PPV、SVV 和 LVeff。MAP 反应者的 NE 前 Ees 较高,VAC 较低。6/8 例 NE 后仍低血压的患者给予多巴酚丁胺。它增加了 Ees、MAP、CI 和 LVeff,同时降低了 HR、Pra 和 VAC。在方案的所有时间点和步骤中,CI 变化与 Pvr 变化成正比,与治疗无关。
基于 SSG 的复苏的心血管反应高度异质,但可通过治疗前的心血管状态测量进行预测。