Department of Surgical Oncology and General Surgery, Key Laboratory of Precision Diagnosis and Treatment of Gastrointestinal Tumors, Ministry of Education, The First Affiliated Hospital of China Medical University, 155 North Nanjing Street, Heping District, Shenyang City 110001, China.
Biomed Res Int. 2021 Mar 28;2021:8852699. doi: 10.1155/2021/8852699. eCollection 2021.
Neoadjuvant (chemo) radiotherapy is used as a standard treatment for locally advanced rectal cancer (LARC), but there is no general consensus on either the efficacy of postoperative adjuvant chemotherapy in patients with LARC after neoadjuvant treatment and surgery, or whether the addition of oxaliplatin to adjuvant chemotherapy provides survival benefits.
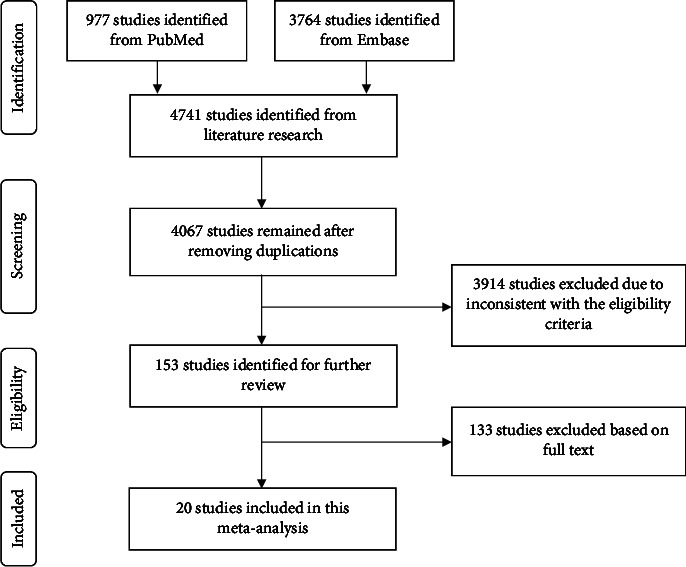
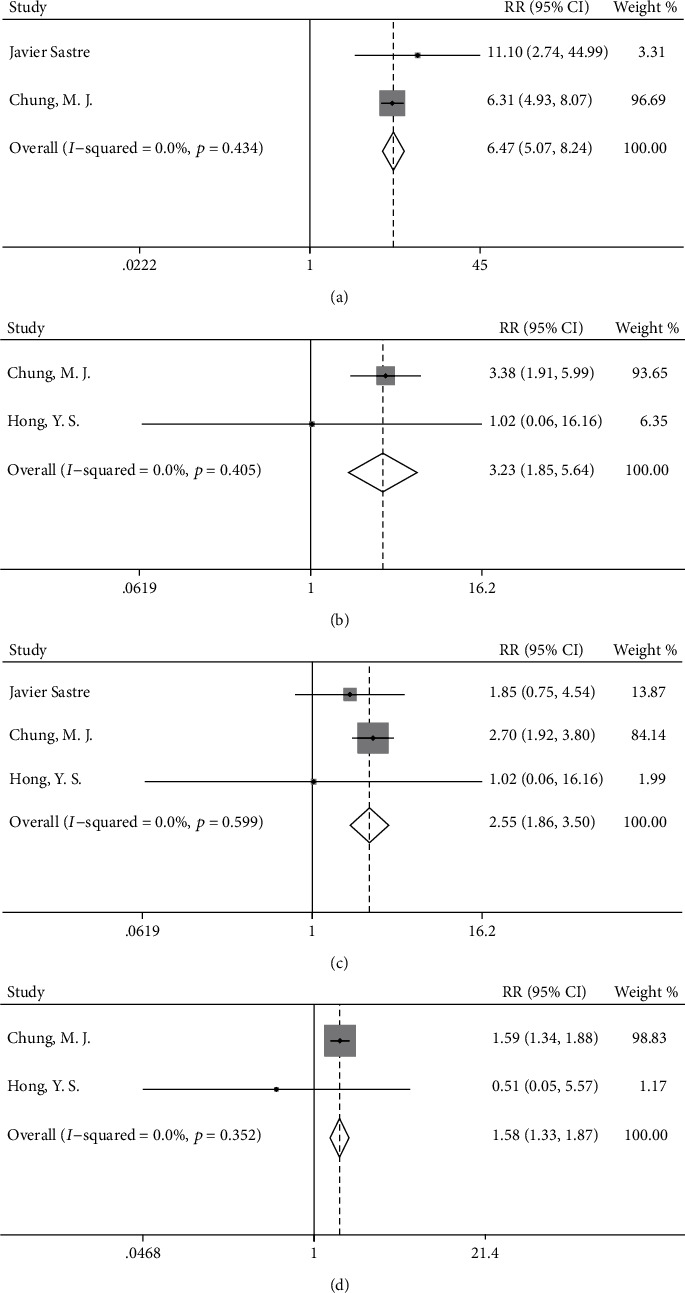
We performed a meta-analysis of data from the PubMed and Embase databases. We included patients with LARC who received neoadjuvant (chemo) radiotherapy and curative surgery. Overall survival (OS), disease-free survival (DFS), toxicity, and compliance were analyzed in the oxaliplatin/fluorouracil- (OX/FU-) based group compared with the FU-based group, and in the chemotherapy group compared with the observation group.
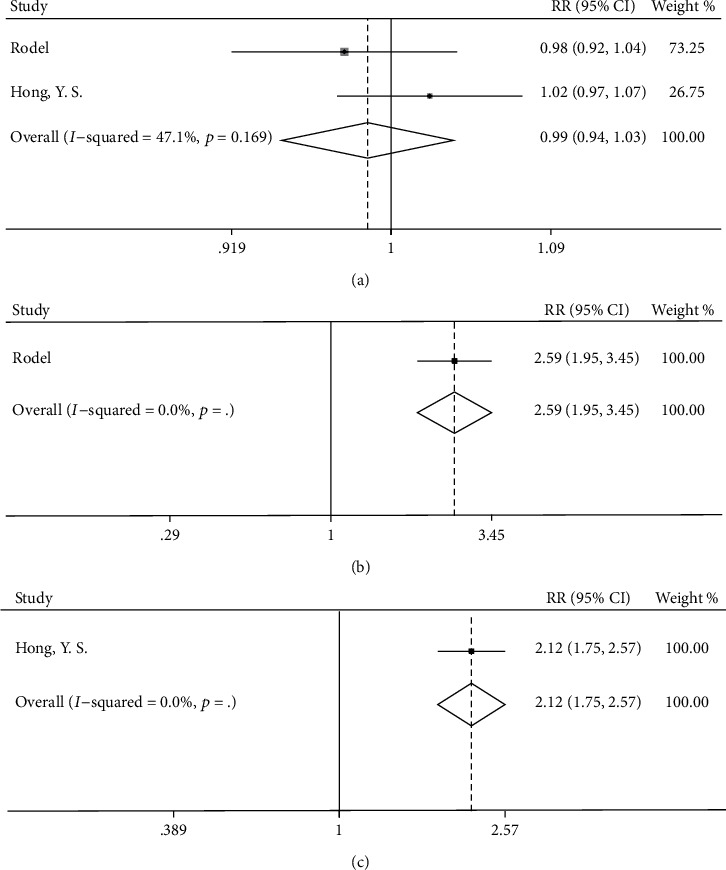
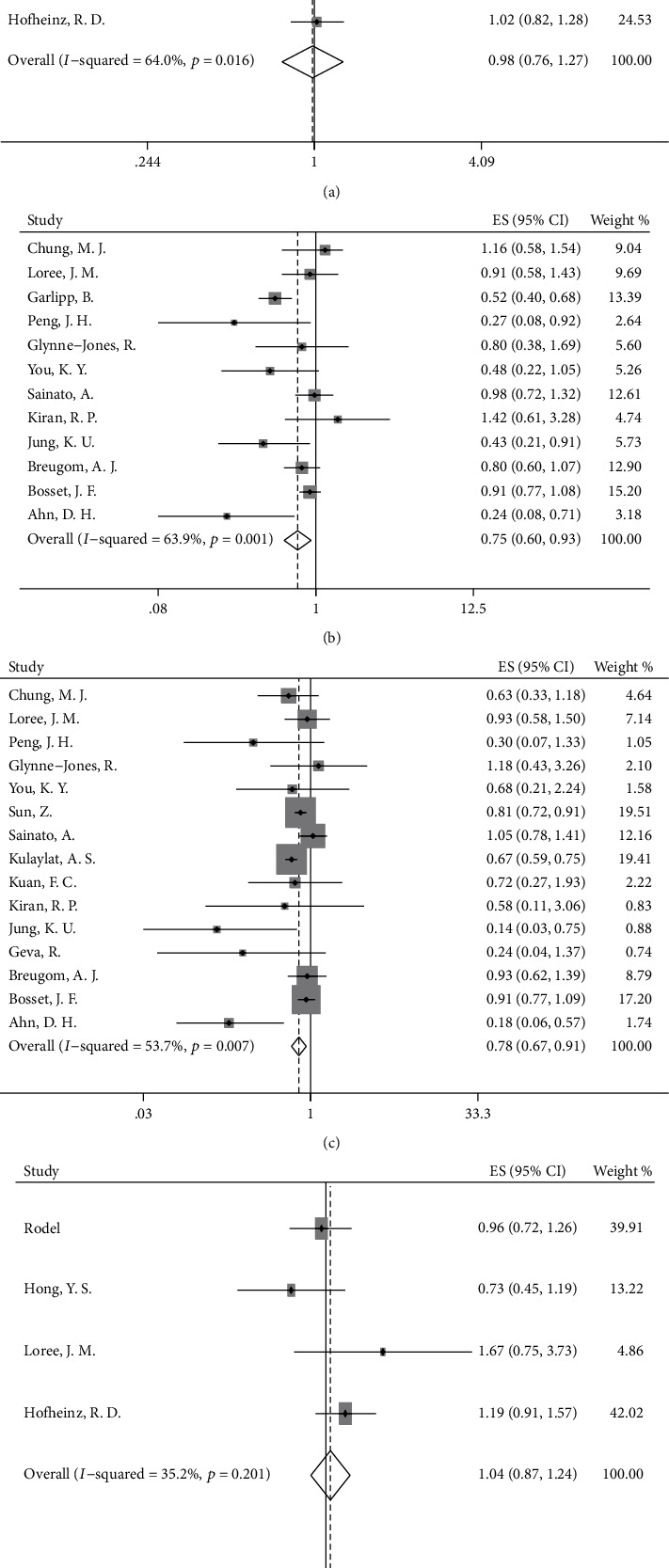
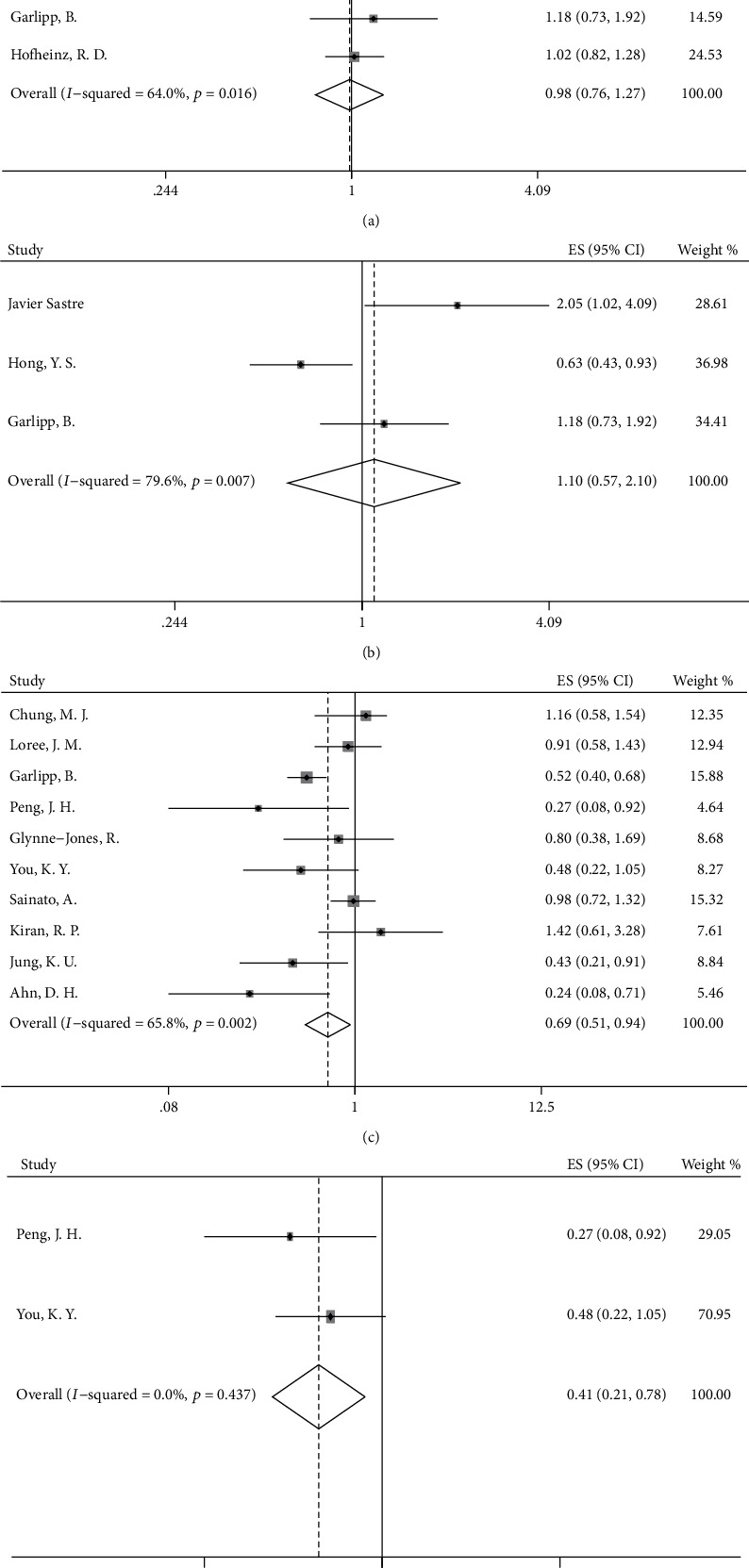
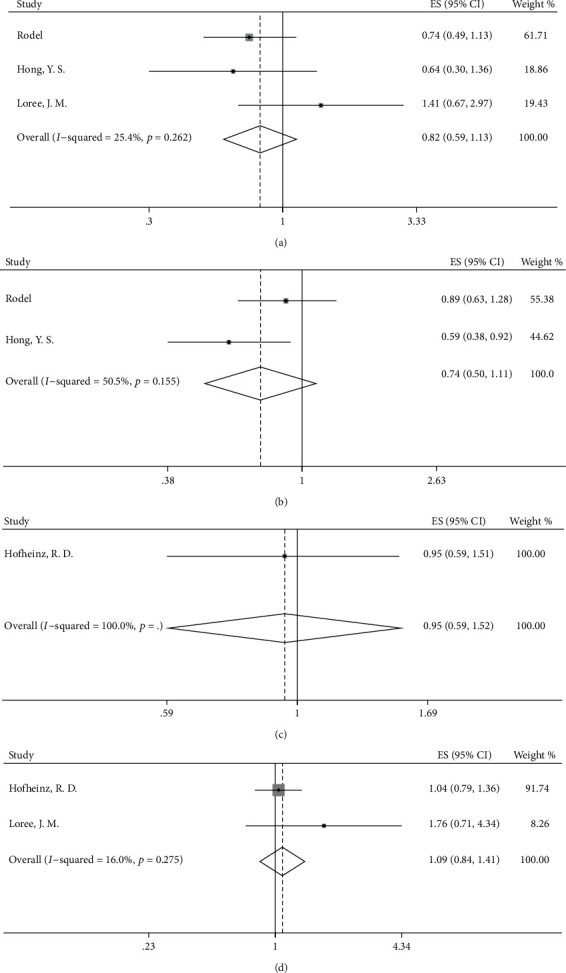
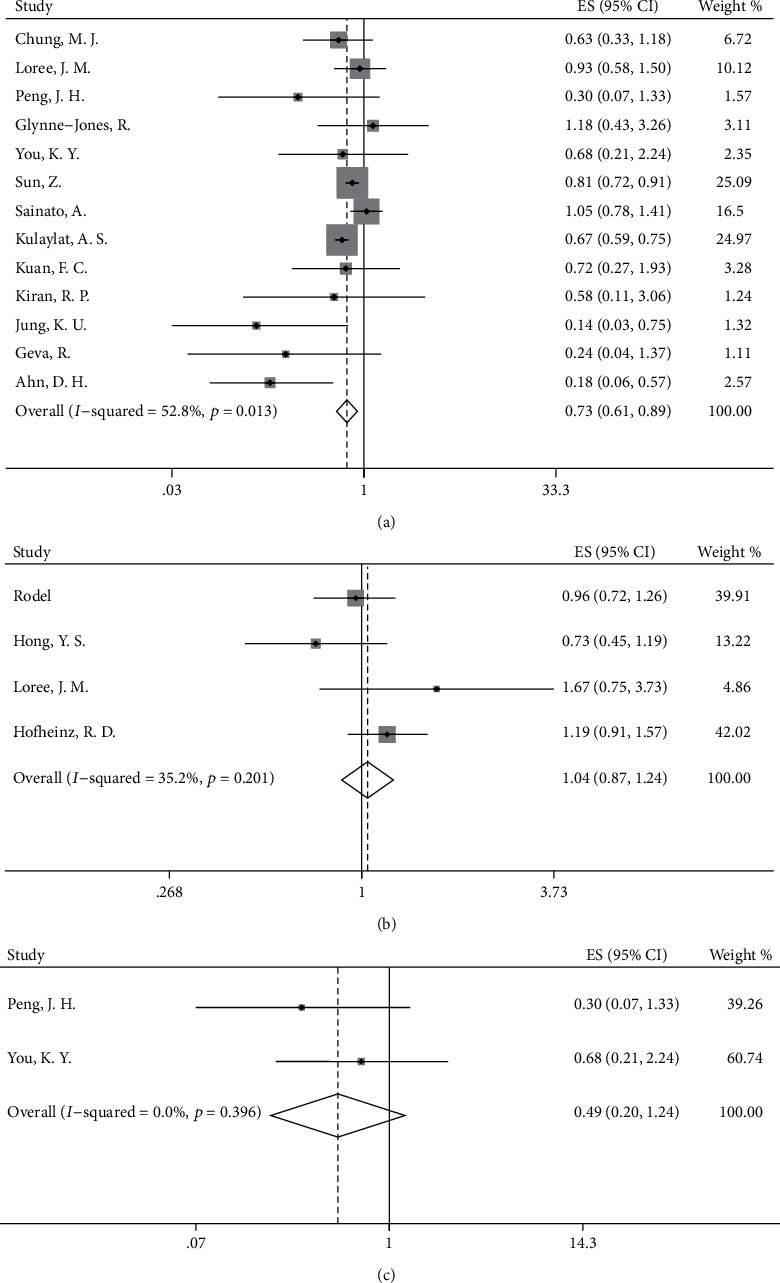
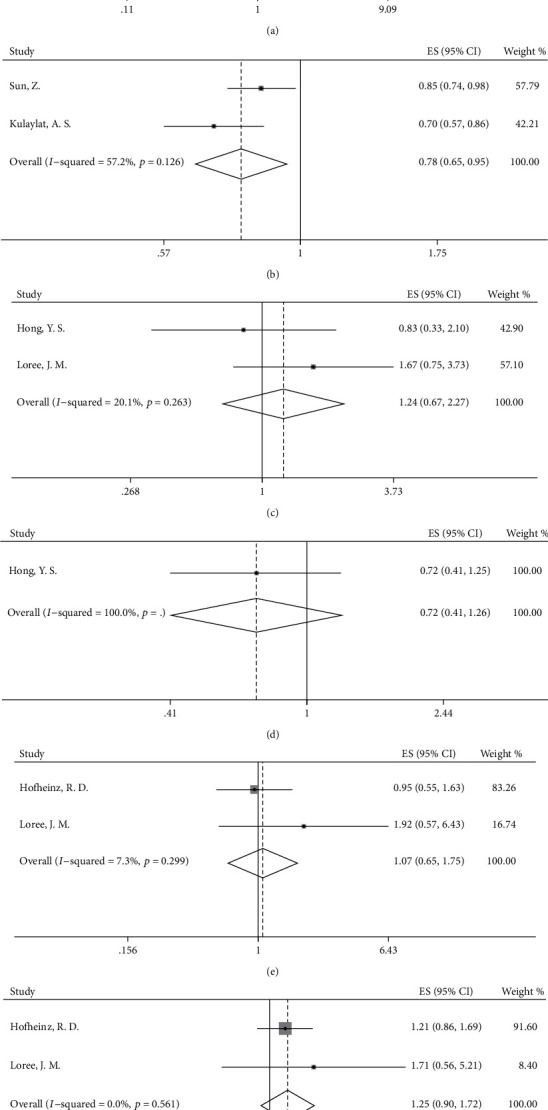
Twenty studies were included in the analysis. Our results indicated that adjuvant chemotherapy prolonged OS (hazard ratio [HR] = 0.78, 95%CI = 0.67-0.91) in patients with LARC treated with neoadjuvant (chemo) radiotherapy and surgery compared with those in the observation group. Subgroup analysis showed the same results in both the ypStage II and ypStage III groups. Compared with those in the observation group, patients in the chemotherapy group also showed an increase in DFS (HR = 0.75, 95%CI = 0.60-0.93). No significant increase was observed in OS (HR = 1.04, 95%CI = 0.87-1.24) or DFS (HR = 0.98, 95%CI = 0.76-1.27) when oxaliplatin was added to FU-based adjuvant chemotherapy, as compared with the FU-based treatment, and subgroup analysis also indicated no survival benefits in the clinical stage II, clinical stage III, ypStage II, and ypStage III groups.
For patients with LARC who have already received neoadjuvant (chemo) radiotherapy and curative surgery, adjuvant chemotherapy improves OS over that in the observation group. Adding oxaliplatin to FU-based adjuvant chemotherapy does not confer survival benefits beyond those from FU-based adjuvant chemotherapy.
新辅助(化疗)放疗被用作局部晚期直肠癌(LARC)的标准治疗方法,但对于接受新辅助治疗和手术的 LARC 患者,术后辅助化疗的疗效,以及是否在辅助化疗中添加奥沙利铂是否可以提供生存获益,尚未达成普遍共识。
我们对 PubMed 和 Embase 数据库中的数据进行了荟萃分析。我们纳入了接受新辅助(化疗)放疗和根治性手术的 LARC 患者。在奥沙利铂/氟尿嘧啶(OX/FU)为基础的组与 FU 为基础的组之间,以及化疗组与观察组之间,分析了总生存(OS)、无病生存(DFS)、毒性和依从性。
共有 20 项研究纳入分析。我们的结果表明,与观察组相比,新辅助(化疗)放疗和手术治疗的 LARC 患者接受辅助化疗可延长 OS(风险比[HR] = 0.78,95%CI = 0.67-0.91)。亚组分析显示,ypStage II 和 ypStage III 组均有相同结果。与观察组相比,化疗组患者的 DFS 也有所提高(HR = 0.75,95%CI = 0.60-0.93)。与 FU 为基础的治疗相比,将奥沙利铂添加到 FU 为基础的辅助化疗中,并未观察到 OS(HR = 1.04,95%CI = 0.87-1.24)或 DFS(HR = 0.98,95%CI = 0.76-1.27)的显著增加,亚组分析也表明在临床分期 II 期、临床分期 III 期、ypStage II 期和 ypStage III 期,没有生存获益。
对于已经接受新辅助(化疗)放疗和根治性手术的 LARC 患者,辅助化疗可改善 OS 优于观察组。在 FU 为基础的辅助化疗中添加奥沙利铂并不能提供优于 FU 为基础的辅助化疗的生存获益。