Nguyen David-Dan, Barber Neil, Bidair Mo, Gilling Peter, Anderson Paul, Zorn Kevin C, Badlani Gopal, Humphreys Mitch, Kaplan Steven, Kaufman Ronald, So Alan, Paterson Ryan, Goldenberg Larry, Elterman Dean, Desai Mihir, Lingeman Jim, Roehrborn Claus, Bhojani Naeem
Faculty of Medicine, McGill University, Montreal, Canada.
Department of Urology, Frimley Park Hospital, Frimley, UK.
Eur Urol Open Sci. 2021 Jan 31;25:21-28. doi: 10.1016/j.euros.2021.01.004. eCollection 2021 Mar.
Surgical options are limited when treating large (>80 cm) prostates for lower urinary tract symptoms (LUTS) due to benign prostatic hyperplasia (BPH). Open simple prostatectomy remains the most common procedure performed for large prostates. There is a need for novel surgical approaches with shorter learning curves and effective treatment. Aquablation could be this novel tool.
To compare the outcome of Aquablation for 30-80-cm prostates with the outcome for 80-150-cm prostates at 2-yr follow-up.
We used data from two trials. WATER is a prospective, double-blind, multicenter, international clinical trial comparing the safety and efficacy of Aquablation and transurethral resection of the prostate in the treatment of LUTS/BPH in men aged 45-80 yr with a prostate of 30-80 cm. WATER II is a prospective, multicenter, single-arm international clinical trial of Aquablation in men with a prostate of 80-150 cm.
Aquablation, an ultrasound-guided, robotically executed waterjet ablative procedure.
We compared 24-mo outcomes between 116 WATER and 101 WATER II study subjects. Student's test or a Wilcoxon test was used to compare continuous variables and Fisher's test for categorical variables.
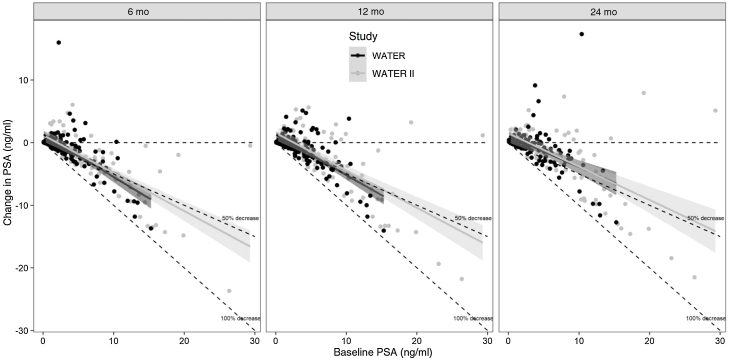
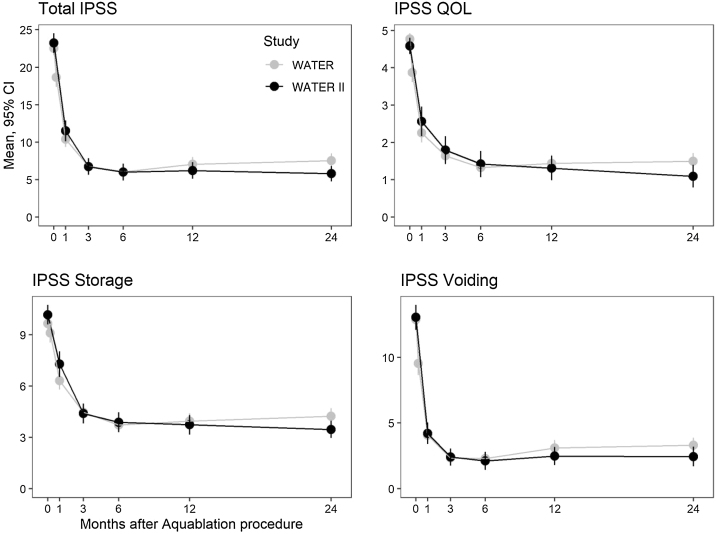
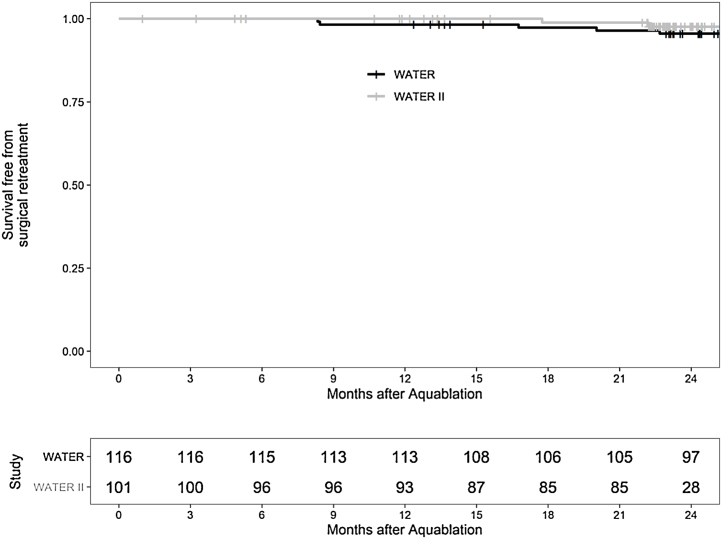
The International Prostate Symptom Score (IPSS) reductions at 24 mo was 14.5 points for WATER and 17.4 points for WATER II ( = 0.31). At baseline, the maximum urinary flow rate (Q) was 9.4 and 8.7 cm/s in WATER and WATER II, improving to 20.5 and 18.2 cm/s, respectively ( = 0.60) at 24 mo. Improvements in both IPSS and Q were immediate and sustained throughout follow-up. At 2 yr, the surgical retreatment rate was 4% in WATER and 2% in WATER II.
Aquablation is effective in patients with a prostate of 30-80 cm and patients with a prostate of 80-150 cm treated for LUTS/BPH, with comparable outcomes in both groups. It has low complication and retreatment rates at 2 yr of follow-up, with durable improvements in functional outcome.
Outcomes of Aquablation for both small-to-moderately-sized and large prostates are similar and sustainable at 2 yr of follow-up.
由于良性前列腺增生(BPH)导致下尿路症状(LUTS)而治疗大体积(>80 cm)前列腺时,手术选择有限。开放性单纯前列腺切除术仍是针对大体积前列腺最常施行的手术。需要具有更短学习曲线且有效的新型手术方法。水消融术可能就是这种新型工具。
比较水消融术治疗30 - 80 cm前列腺与治疗80 - 150 cm前列腺在2年随访时的结果。
设计、地点与参与者:我们使用了两项试验的数据。WATER是一项前瞻性、双盲、多中心、国际临床试验,比较水消融术与经尿道前列腺切除术治疗45 - 80岁、前列腺体积为30 - 80 cm的男性LUTS/BPH的安全性和有效性。WATER II是一项针对前列腺体积为80 - 150 cm男性的水消融术的前瞻性、多中心、单臂国际临床试验。
水消融术,一种超声引导、机器人执行的水刀消融手术。
我们比较了116名WATER研究对象和101名WATER II研究对象的24个月结果。采用学生t检验或威尔科克森检验比较连续变量,采用费舍尔检验比较分类变量。
WATER组在24个月时国际前列腺症状评分(IPSS)降低了14.5分,WATER II组降低了17.4分(P = 0.31)。基线时,WATER组和WATER II组的最大尿流率(Q)分别为9.4和8.7 cm/s,在24个月时分别提高到20.5和18.2 cm/s(P = 0.60)。IPSS和Q的改善在整个随访期间都是即时且持续的。在2年时,WATER组的手术再治疗率为4%,WATER II组为2%。
水消融术对于治疗LUTS/BPH的30 - 80 cm前列腺患者和80 - 150 cm前列腺患者均有效,两组结果相当。在2年随访时并发症和再治疗率较低,功能结局有持久改善。
水消融术治疗小至中等体积和大体积前列腺的结果在2年随访时相似且可持续。