Hoekstra Robert J, Goossens Ward J H, Beulens Alexander, van Herk Hilde, Hoevenaars Brigiet M, de Baaij Joost, Somford Diederik M, Sedelaar J P Michiel, van Basten Jean-Paul A, Vrijhof H J Eric J
Department of Urology, Catharina Hospital Eindhoven, Eindhoven, The Netherlands.
Department of Urology, Canisius Wilhelmina Hospital, Nijmegen, The Netherlands.
Eur Urol Open Sci. 2021 Apr 27;28:36-42. doi: 10.1016/j.euros.2021.04.003. eCollection 2021 Jun.
The minimum volume standard is 100 robot-assisted radical prostatectomy (RARP) procedures per hospital in the Netherlands, so patients have to be referred to high-volume surgical centers for RARP. During preoperative work-up, prostate biopsies taken elsewhere are reassessed, with upgrading or downgrading of the initial Gleason grade group a possible consequence.
To determine if prostate biopsy reassessment leads to adjustment of the surgical plan regarding a nerve-sparing approach and extended pelvic lymph node dissection (ePLND) during RARP.
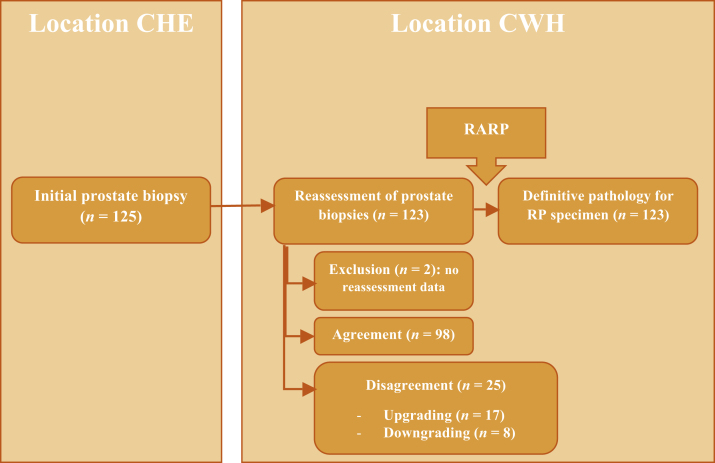
For 125 men who were referred to the Prosper prostate center at Canisius Wilhelmina Hospital (CWH) in the Netherlands between 2013 and 2016, results for the initial assessment of prostate biopsy by a local uropathologist were compared to results for biopsy reassessment by dedicated uropathologists at CWH.
The pathologists reached agreement in 80% of the cases. In cases for which there was disagreement ( = 25), biopsy revision involved upgrading of the initial grade group in 68% and downgrading in 32%. Biopsy reassessment led to a change in surgical plan in ten cases (8%). As a result of upgrading, ePLND was performed in three patients (2%). ePLND was omitted in one patient (1%) because of downgrading. For three patients (2%) a non-nerve-sparing procedure was planned after upgrading of the initial grade group. For four patients (3%), a unilateral nerve-sparing procedure was performed after downgrading.
This study shows that there is large interobserver agreement between uropathologists in the assessment of Gleason grade group in prostate biopsy specimens. Reassessment rarely leads to a change in surgical plan regarding the indication for a nerve-sparing approach and ePLND. Therefore, reassessment of prostate biopsy before radical prostatectomy can be omitted when the initial pathological assessment was performed by a dedicated uropathologist.
Reassessment of the initial prostate biopsy specimen for patients referred to a specialist center for robot-assisted removal of the prostate rarely influences surgical planning and can be omitted.
在荷兰,每家医院机器人辅助根治性前列腺切除术(RARP)的最低手术量标准是100例,因此患者必须被转诊至高手术量的外科中心进行RARP。在术前检查期间,会重新评估在其他地方所取的前列腺活检样本,这可能会导致最初的 Gleason 分级组出现升级或降级。
确定前列腺活检重新评估是否会导致RARP期间关于保留神经方法和扩大盆腔淋巴结清扫术(ePLND)的手术计划调整。
设计、地点和参与者:对2013年至2016年间转诊至荷兰卡尼修斯·威廉明娜医院(CWH)的普罗斯珀前列腺中心的125名男性患者,将当地泌尿病理学家对前列腺活检的初始评估结果与CWH的专业泌尿病理学家对活检重新评估的结果进行比较。
病理学家在80%的病例中达成了一致。在存在分歧的病例(n = 25)中,活检结果修正涉及68%的病例初始分级组升级,32%的病例降级。活检重新评估导致10例(8%)手术计划改变。由于升级,3例患者(2%)进行了ePLND。1例患者(1%)因降级而未进行ePLND。对于3例患者(2%),在初始分级组升级后计划进行非保留神经手术。对于4例患者(3%),在降级后进行了单侧保留神经手术。
本研究表明,泌尿病理学家在评估前列腺活检标本的Gleason分级组方面存在较大的观察者间一致性。重新评估很少导致关于保留神经方法和ePLND指征的手术计划改变。因此,当初始病理评估由专业泌尿病理学家进行时,根治性前列腺切除术前行前列腺活检重新评估可省略。
转诊至专科中心进行机器人辅助前列腺切除术的患者,对初始前列腺活检标本的重新评估很少影响手术规划,可省略。