Kumar Abhishek, Cherry Daniel R, Courtney Patrick T, Nalawade Vinit, Kotha Nikhil, Riviere Paul J, Efstathiou Jason, McKay Rana R, Karim Kader A, Rose Brent S, Stewart Tyler F
Department of Radiation Medicine and Applied Sciences, University of California San Diego, La Jolla, CA, USA.
Department of Radiation Oncology, Harvard, Cambridge, MA, USA.
Eur Urol Open Sci. 2021 Jun 9;30:1-10. doi: 10.1016/j.euros.2021.05.009. eCollection 2021 Aug.
Muscle-invasive bladder cancer (MIBC) remains undertreated despite multiple potentially curative options. Both radical cystectomy (RC) with or without neoadjuvant chemotherapy and trimodal therapy (TMT), including transurethral resection of bladder tumor followed by chemoradiotherapy, are standard treatments.
To evaluate real-world clinical outcomes of RC with neoadjuvant chemotherapy (RC-NAC), RC without NAC, TMT with National Comprehensive Cancer Network guideline-preferred radiosensitizing chemotherapy including cisplatin or mitomycin-C and 5-fluorouracil (pTMT), and TMT with nonpreferred chemotherapy (npTMT).
US veterans with nonmetastatic MIBC (T2-4aN0-3M0) were studied.
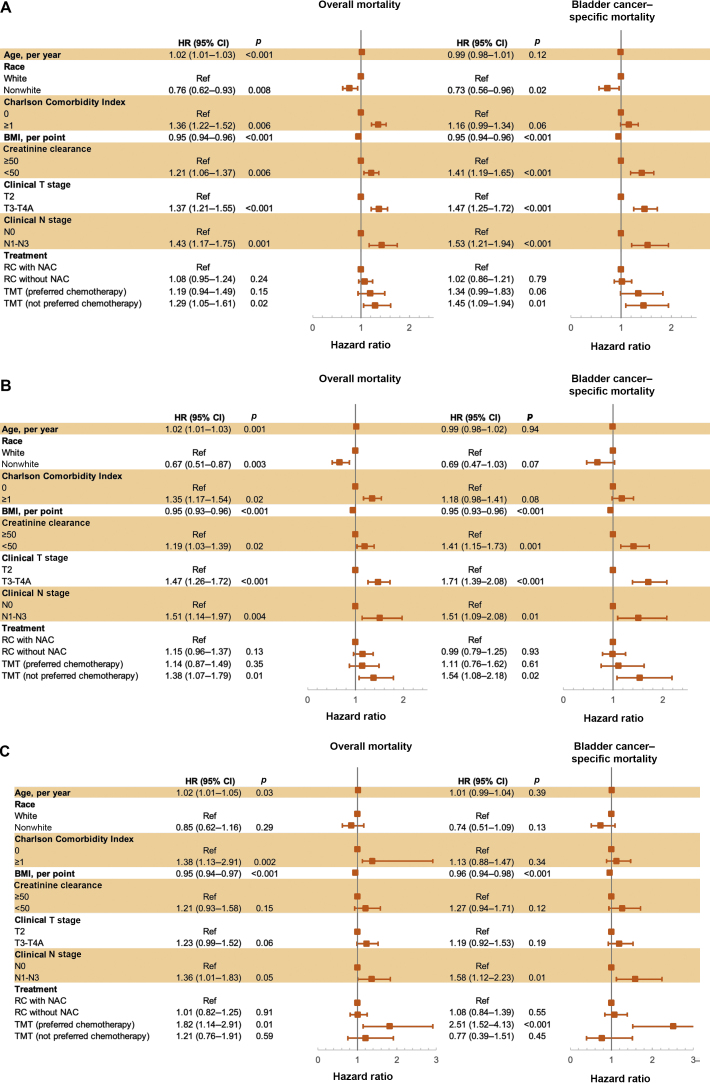
Overall mortality (OM) was evaluated with multivariable Cox proportional hazard model. Bladder cancer-specific mortality (BCSM) was evaluated with multivariable Fine-Gray regression. Salvage cystectomy rates were obtained by chart review.
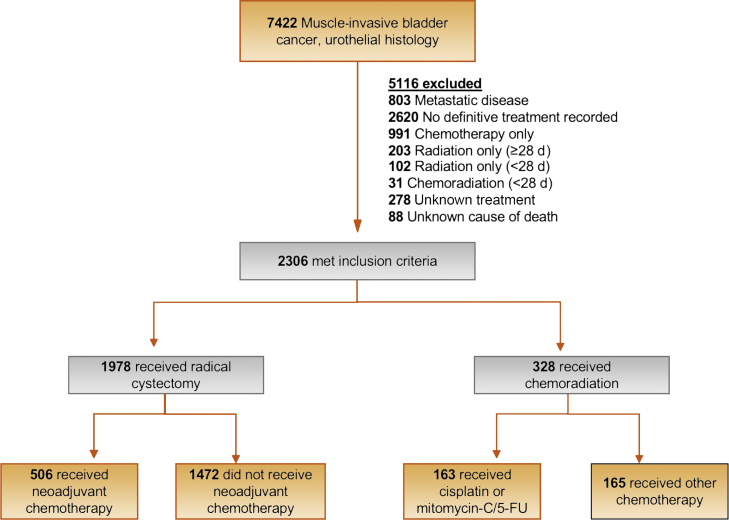
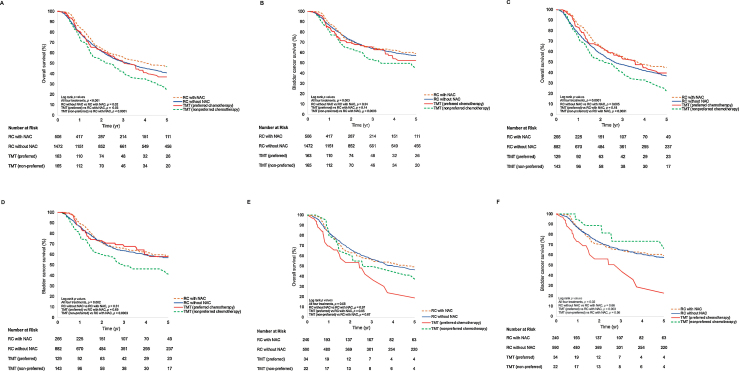
Overall 2306 patients were included: 1472 (64%) with RC without NAC, 506 (22%) with RC-NAC, 163 (7%) with pTMT, and 165 (7%) with npTMT. On multivariable analysis, pTMT was associated with similar OM (hazard ratio [HR] 1.19; 95% confidence interval [CI] 0.94-1.50; = 0.15) and BCSM (HR 1.34; 95% CI 0.99-1.83; = 0.06) to RC-NAC; npTMT was associated with worse OM (HR 1.30; 95% CI 1.04-1.61; = 0.02) and BCSM (HR 1.45; 95% CI 1.09-1.94; = 0.01). RC without NAC was associated with similar OM (HR 1.08; 95% CI 0.95-1.24; = 0.24) and BCSM (HR 1.02; 95% CI 0.86-1.21; = 0.79). When stratified by age, among patients ≥65 yr of age, treatment with pTMT was associated with similar OM (HR 1.14; 95% CI 0.87-1.50; = 0.35) and BCSM (HR 1.11; 95% CI 0.76-1.62; = 0.60). Among patients <65 yr of age, pTMT was associated with worse OM (HR 1.82; 95% CI 1.14-2.91; = 0.01) and BCSM (HR 2.51; 95% CI 1.52-4.13; < 0.01). The 5-yr cumulative incidence of salvage cystectomy in the TMT group was 3.6%.
In MIBC, patients receiving pTMT have comparable survival in RC-NAC patients ≥65 yr and inferior survival in RC-NAC patients <65 yr. Salvage cystectomy rates were low.
Management of muscle-invasive bladder cancer is a multidisciplinary effort requiring thoughtful discussions with patients about treatment options, including trimodal therapy, which is an effective treatment option.
尽管有多种潜在的治愈性选择,但肌肉浸润性膀胱癌(MIBC)的治疗仍不充分。根治性膀胱切除术(RC)无论是否联合新辅助化疗,以及三联疗法(TMT),包括经尿道膀胱肿瘤切除术后续放化疗,都是标准治疗方法。
评估接受新辅助化疗的根治性膀胱切除术(RC-NAC)、未接受新辅助化疗的根治性膀胱切除术(RC)、采用美国国立综合癌症网络指南推荐的包括顺铂或丝裂霉素-C及5-氟尿嘧啶的放射增敏化疗的三联疗法(pTMT),以及采用非推荐化疗的三联疗法(npTMT)的真实世界临床结局。
设计、背景与参与者:对美国患有非转移性MIBC(T2-4aN0-3M0)的退伍军人进行研究。
采用多变量Cox比例风险模型评估总死亡率(OM)。采用多变量Fine-Gray回归评估膀胱癌特异性死亡率(BCSM)。通过查阅病历获得挽救性膀胱切除术率。
共纳入2306例患者:1472例(64%)接受未行新辅助化疗的根治性膀胱切除术,506例(22%)接受新辅助化疗的根治性膀胱切除术,163例(7%)接受pTMT,165例(7%)接受npTMT。多变量分析显示,pTMT与RC-NAC的OM(风险比[HR]1.19;95%置信区间[CI]0.94-1.50;P=0.15)和BCSM(HR1.34;95%CI0.99-1.83;P=0.06)相似;npTMT与更差的OM(HR1.30;95%CI1.04-1.61;P=0.02)和BCSM(HR1.45;95%CI1.09-1.94;P=0.01)相关。未行新辅助化疗的根治性膀胱切除术与OM(HR1.08;95%CI0.95-1.24;P=0.24)和BCSM(HR1.02;95%CI0.86-1.21;P=0.79)相似。按年龄分层时,在≥65岁的患者中,pTMT治疗与OM(HR1.14;95%CI0.87-1.50;P=0.35)和BCSM(HR1.11;95%CI0.76-1.62;P=0.60)相似。在<65岁的患者中,pTMT与更差的OM(HR1.82;95%CI1.14-2.91;P=0.01)和BCSM(HR2.51;95%CI1.52-4.13;P<0.01)相关。TMT组挽救性膀胱切除术的5年累积发生率为3.6%。
在MIBC中,接受pTMT的患者在≥65岁的RC-NAC患者中生存率相当,而在<65岁的RC-NAC患者中生存率较差。挽救性膀胱切除术率较低。
肌肉浸润性膀胱癌的管理是一项多学科工作,需要与患者认真讨论治疗选择,包括三联疗法,这是一种有效的治疗选择。