Department of Cardiology, Peking University First Hospital, No.8 Xishiku Street, Xicheng District, Beijing, 100034, China.
BMC Cardiovasc Disord. 2021 Aug 3;21(1):372. doi: 10.1186/s12872-021-02165-5.
Complete atrioventricular block (AVB) is a life-threatening condition that usually occurs in elderly people with organic heart disease. We herein describe a rare case of complete AVB in a young man with hypertrophic obstructive cardiomyopathy (HOCM) complicated by cholecystitis and cholangitis. Both cardio-biliary reflex and alcohol septal ablation (ASA) can cause conduction block, but the latter is often irreversible. However, their simultaneous occurrence in a patient has not been reported.
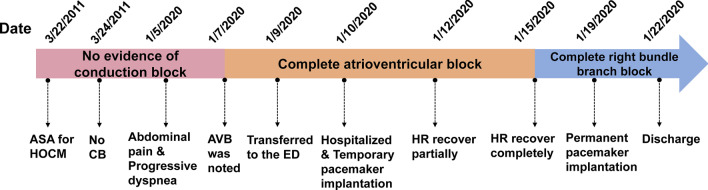
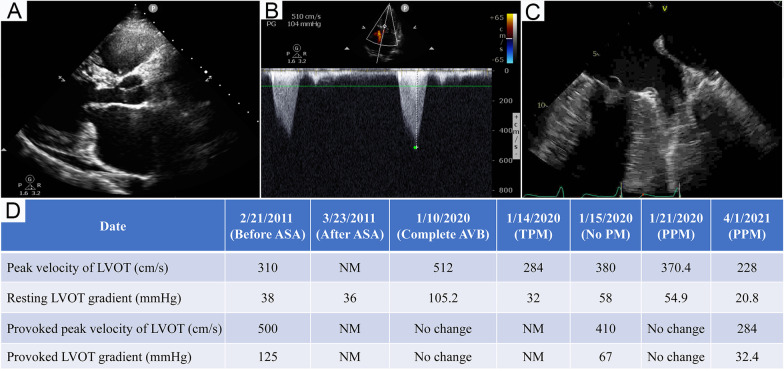
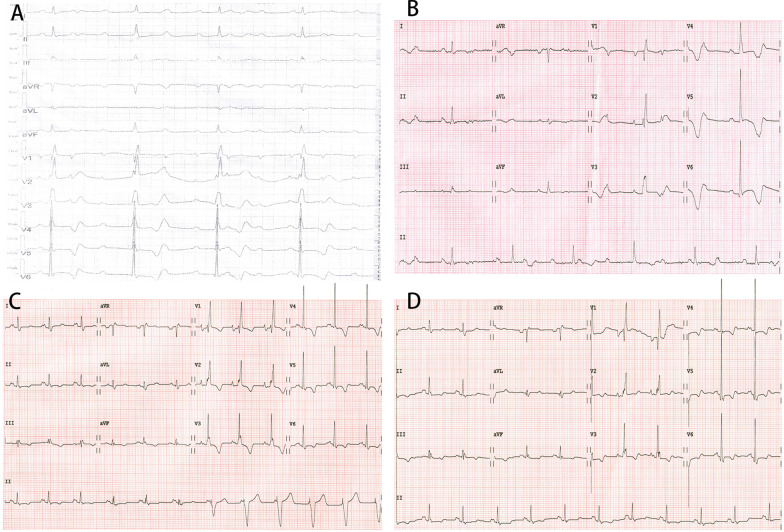
A 31-year-old man presented with acute cholecystitis and cholangitis and complete AVB, which had been diagnosed at a local hospital on the third day after onset. On the fourth day, he was transferred to the emergency department of our hospital because of persistent complete AVB, although his abdominal pain had been partially relieved. An echocardiogram showed a remarkably elevated left ventricular outflow tract (LVOT) gradient (105.2 mmHg) despite the performance of ASA 9 years previously. The abdominal pain gradually disappeared, and normal sinus rhythm was completely recovered 11 days after onset. We determined that cardio-biliary reflex was the cause of the AVB because of the absence of other common causes. Finally, the patient underwent implantation of a permanent pacemaker to reduce the LVOT obstruction and avoid the risk of AVB recurrence.
Cholecystitis is a rare cause of complete AVB, which is a difficult differential diagnosis when complicated by HOCM after ASA. Clinicians should be alert to the possibility of cholecystitis in patients with abdominal pain and an unknown cause of bradycardia, complete AVB, or even sinus arrest.
完全性房室传导阻滞(AVB)是一种危及生命的病症,通常发生在患有器质性心脏病的老年人群中。本文报告了一例罕见的肥厚型梗阻性心肌病(HOCM)合并胆囊炎和胆管炎的年轻男性完全性 AVB 病例。心胆反射和酒精室间隔消融术(ASA)均可引起传导阻滞,但后者通常是不可逆的。然而,它们同时发生在同一患者中尚未见报道。
一名 31 岁男性因急性胆囊炎和胆管炎并发完全性 AVB 于发病后第 3 天在当地医院就诊。发病第 4 天,尽管腹痛部分缓解,但因持续性完全性 AVB 转至我院急诊科。超声心动图显示左心室流出道(LVOT)梯度显著升高(105.2mmHg),尽管 9 年前曾行 ASA。腹痛逐渐消失,发病 11 天后完全恢复窦性心律。我们确定心胆反射是 AVB 的原因,因为没有其他常见的原因。最终,患者接受了永久性起搏器植入术以减轻 LVOT 梗阻并避免 AVB 复发的风险。
胆囊炎是完全性 AVB 的罕见病因,当 ASA 后并发 HOCM 时,这是一种难以鉴别的诊断。当出现不明原因的心动过缓、完全性 AVB 甚至窦性停搏时,临床医生应警惕胆囊炎的可能性。