Department of Obstetrics and Gynecology, Peking University People's Hospital, Beijing, 100044, China.
Reproductive Medical Center, Peking University People's Hospital, Beijing, 100044, China.
Reprod Biol Endocrinol. 2021 Aug 3;19(1):118. doi: 10.1186/s12958-021-00808-y.
Fertility-sparing therapy is an alternative conservative treatment for patients with early stage endometrioid cancer or atypical endometrial hyperplasia. In this study, we investigated pregnancy outcomes and pregnancy-associated factors in young patients receiving hormonal therapy.
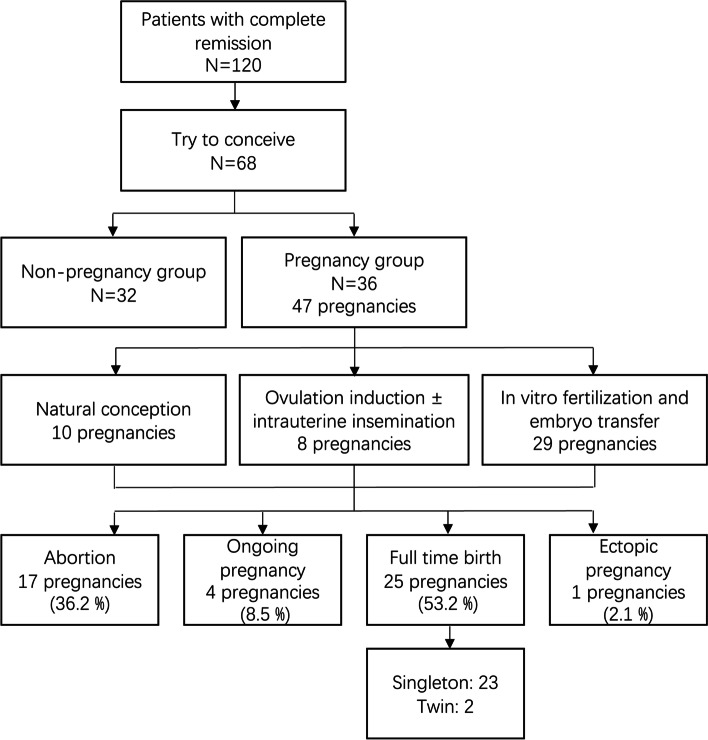
We retrospectively analyzed 68 patients who attempted to conceive after fertility-sparing therapy and achieving complete remission (CR). They were divided into a pregnancy group and a non-pregnancy group. A Cox proportional hazard regression model was applied for univariate and multivariate analysis to determine factors associated with pregnancy. Kaplan-Meier analysis, combined with the log-rank test, was used to calculate a patient's pregnancy probability and the distribution of recurrence-free survival (RFS).
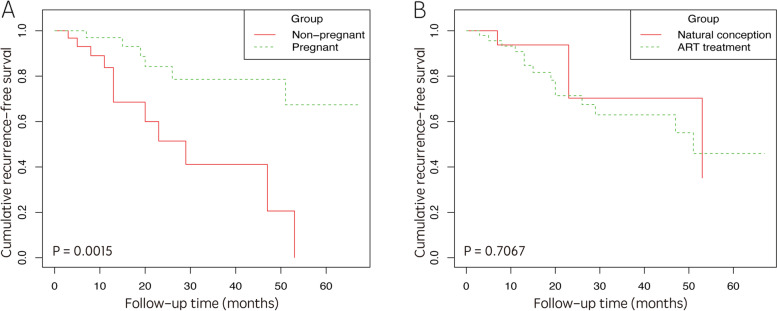
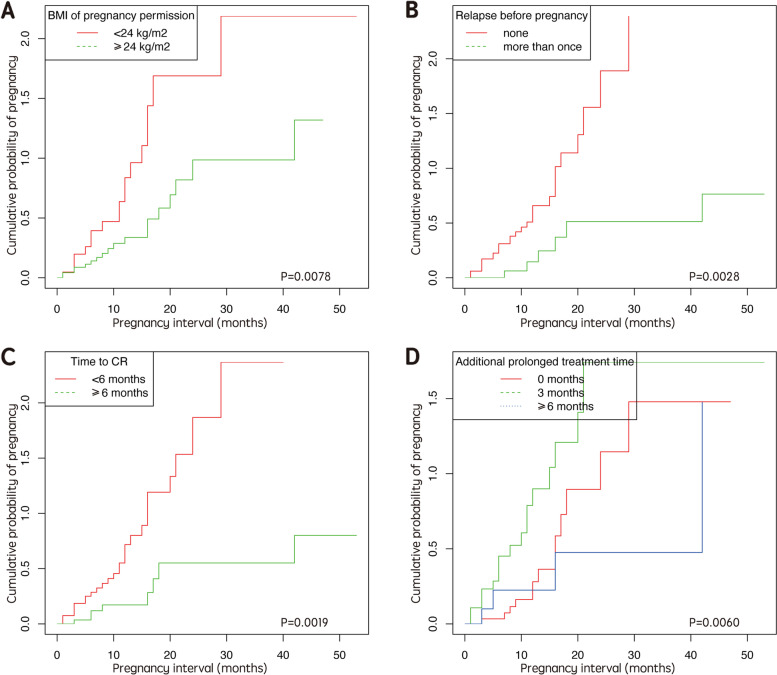
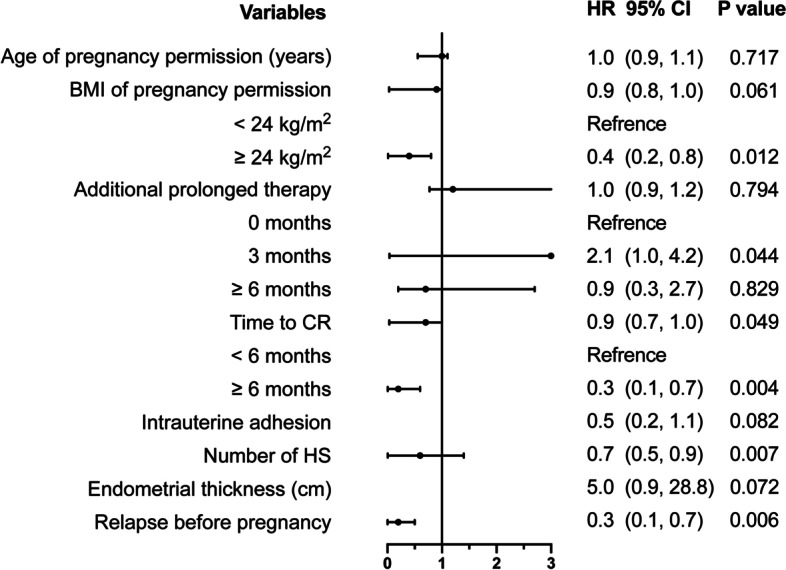
A total of 36 patients became pregnant with 47 pregnancies. Univariate and multivariate Cox analysis revealed that several factors were associated with pregnancy, including BMI at the time of pregnancy permission, the time to CR, prolonged treatment time, the number of hysteroscopy procedures, the endometrium thickness after CR, and relapse before pregnancy. The mean RFS of patients who achieved pregnancy, and those who did not, was 27.6 months and 14.8 months, respectively (P = 0.002). No significant difference was detected in terms of cumulative RFS when compared between assisted reproductive technology (ART) cases and those involving natural conception (NC) (P = 0.707).
Normal BMI, a shorter time to CR, a prolonged three-month treatment, fewer hysteroscopy procedures, and a thicker endometrium may be positive indicators for successful pregnancies, while relapse before pregnancy may have a negative effect on conception. Moreover, a successful pregnancy protects the endometrium while ART does not increase the risk of recurrence.
保留生育功能疗法是治疗早期子宫内膜样癌或非典型子宫内膜增生患者的一种替代保守治疗方法。在这项研究中,我们研究了接受激素治疗的年轻患者妊娠结局和与妊娠相关的因素。
我们回顾性分析了 68 例接受保留生育功能治疗并达到完全缓解(CR)后尝试妊娠的患者。他们被分为妊娠组和非妊娠组。应用 Cox 比例风险回归模型进行单因素和多因素分析,以确定与妊娠相关的因素。Kaplan-Meier 分析结合对数秩检验用于计算患者的妊娠概率和无复发生存(RFS)分布。
共有 36 例患者妊娠,共 47 次妊娠。单因素和多因素 Cox 分析显示,妊娠与多个因素相关,包括妊娠许可时的 BMI、达到 CR 的时间、治疗时间延长、宫腔镜检查次数、CR 后子宫内膜厚度以及妊娠前复发。妊娠组和未妊娠组的平均 RFS 分别为 27.6 个月和 14.8 个月(P=0.002)。辅助生殖技术(ART)和自然受孕(NC)的累积 RFS 无显著差异(P=0.707)。
正常 BMI、较短的达到 CR 的时间、延长的三个月治疗、较少的宫腔镜检查次数和较厚的子宫内膜可能是成功妊娠的积极指标,而妊娠前的复发可能对受孕产生负面影响。此外,成功妊娠可以保护子宫内膜,而 ART 不会增加复发风险。