OPEN, Institute of Clinical Research, University of Southern Denmark, Odense, Denmark
Bandim Health Project, Bissau, Guinea-Bissau.
BMJ Glob Health. 2021 Aug;6(8). doi: 10.1136/bmjgh-2021-006127.
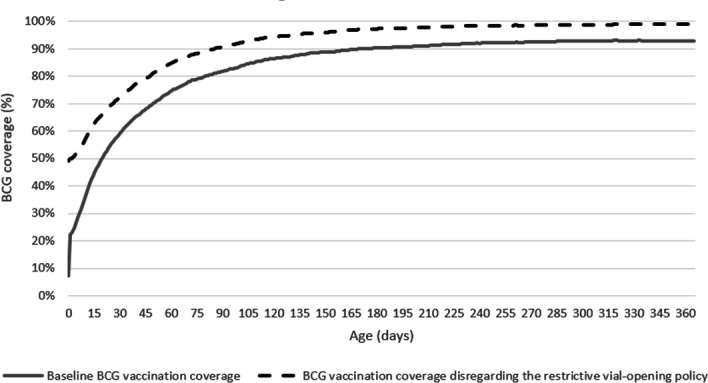
BCG vaccination is frequently delayed in low-income countries. Restrictive vial-opening policies, where a vial of BCG vaccine is not opened for few children, are a major reason for delay. During delays, children are unprotected against tuberculosis (TB) and deprived of non-specific effects of BCG. We assessed the potential effect and cost-effectiveness of disregarding the restrictive vial-opening policy, on TB and all-cause mortality, in children aged 0-4 years in Guinea-Bissau.
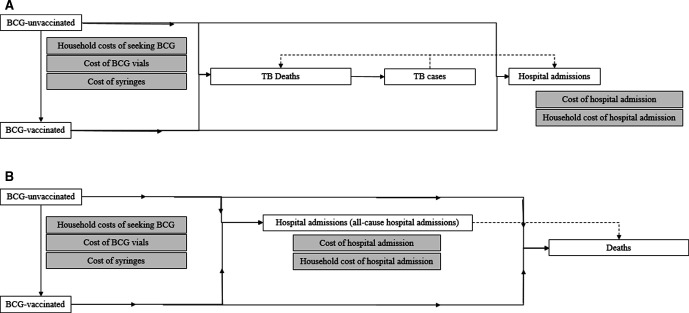
Using static mathematical models, we estimated the absolute and percentage change in TB and all-cause deaths, in children aged 0-4 years, between the current BCG vaccine restrictive-opening policy scenario, and a non-restrictive policy scenario where all children were vaccinated in the first health-facility contact. Incremental cost-effectiveness was estimated by integration of vaccine and treatment costs.
Disregarding the restrictive BCG vial-opening policy was estimated to reduce TB deaths by 11.0% (95% uncertainty range (UR):0.5%-28.8%), corresponding to 4 (UR:0-15) TB deaths averted per birth cohort in Guinea-Bissau, resulting in incremental cost-effectiveness of US$ 911 per discounted life-year gained (LYG) (UR:145-9142). For all-cause deaths, the estimated reduction was 8.1% (UR: 3.3%-12.7%) corresponding to 392 (UR:158-624) fewer all-cause deaths and an incremental cost-effectiveness of US$ 9 (UR:5-23) per discounted LYG.
Disregarding the restrictive BCG vial-opening policy was associated with reductions in TB deaths and all-cause deaths and low cost-effectiveness ratios. Our results suggest that it would be cost-effective to disregard the restrictive vial-opening policy. Other settings with similar practice are also likely to gain from disregarding this policy.
在低收入国家,卡介苗(BCG)接种经常被延迟。小瓶开启政策限制,即一个小瓶 BCG 疫苗只为少数儿童开启,是延迟的主要原因。在延迟期间,儿童无法免受结核病(TB)的侵害,也无法获得 BCG 的非特异性作用。我们评估了在几内亚比绍,忽略小瓶开启政策对 0-4 岁儿童的 TB 和全因死亡率的潜在影响和成本效益。
我们使用静态数学模型,估计当前 BCG 疫苗限制开启政策情景与非限制政策情景(所有儿童在首次医疗接触时接种疫苗)之间,0-4 岁儿童的 TB 和全因死亡的绝对和百分比变化。通过整合疫苗和治疗成本,估算增量成本效益。
忽略限制 BCG 小瓶开启政策估计可减少 11.0%的 TB 死亡(95%置信区间(UR):0.5%-28.8%),相当于在几内亚比绍,每出生队列可避免 4 例(UR:0-15 例)TB 死亡,增量成本效益为每获得一个贴现生命年(LYG)911 美元(UR:145-9142 美元)。对于全因死亡,估计减少 8.1%(UR:3.3%-12.7%),相当于可减少 392 例(UR:158-624 例)全因死亡,增量成本效益为每获得一个贴现 LYG9 美元(UR:5-23 美元)。
忽略限制 BCG 小瓶开启政策与减少 TB 死亡和全因死亡以及低成本效益比相关。我们的研究结果表明,忽略这种限制小瓶开启政策可能具有成本效益。其他具有类似做法的环境也可能受益于忽略这一政策。