Siafis Spyridon, Rodolico Alessandro, Çıray Oğulcan, Murphy Declan G, Parellada Mara, Arango Celso, Leucht Stefan
Department of Psychiatry and Psychotherapy, School of Medicine, Technical University of Munich, 81675 Munich, Germany.
Department of Experimental and Clinical Medicine, Psychiatric Clinic University Hospital 'Gaspare Rodolico', University of Catania, 95125 Catania, Italy.
Brain Sci. 2021 Jul 9;11(7):908. doi: 10.3390/brainsci11070908.
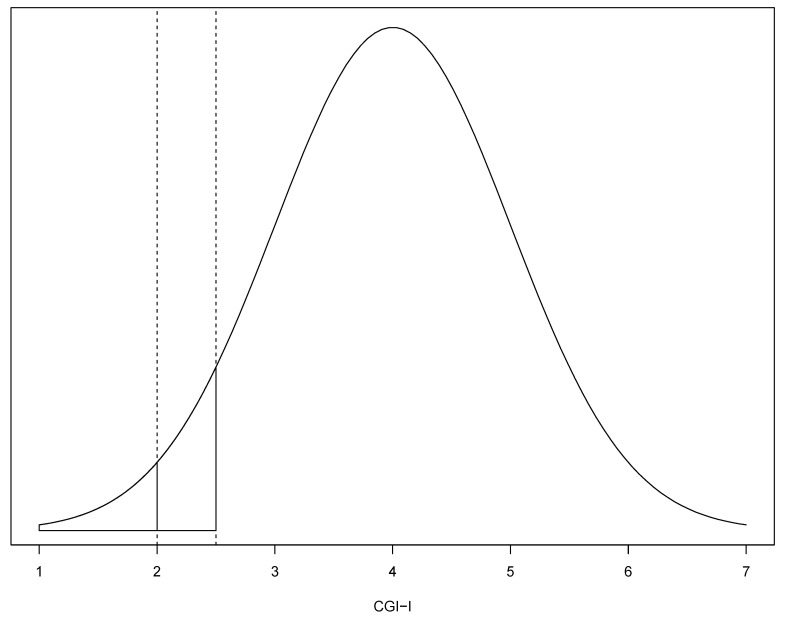
Response to treatment, according to Clinical Global Impression-Improvement (CGI-I) scale, is an easily interpretable outcome in clinical trials of autism spectrum disorder (ASD). Yet, the CGI-I rating is sometimes reported as a continuous outcome, and converting it to dichotomous would allow meta-analysis to incorporate more evidence.
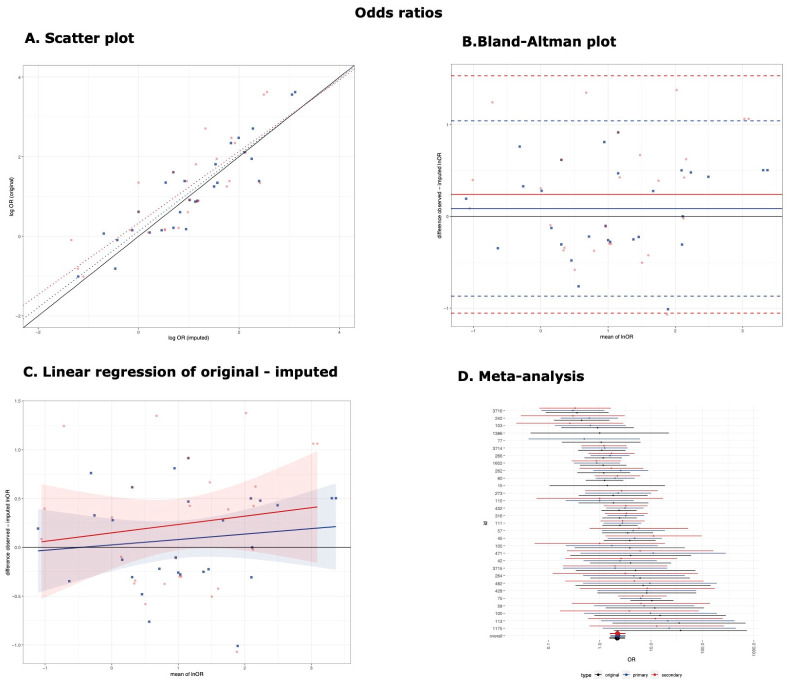
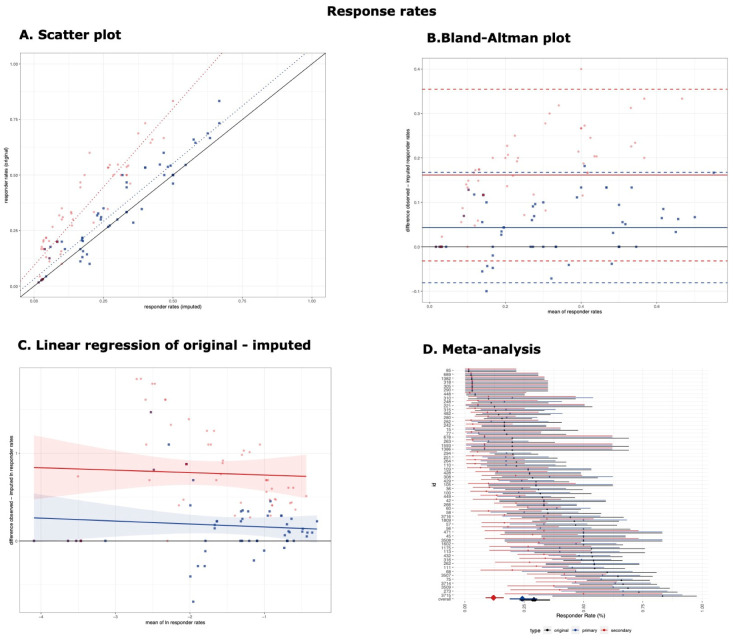
Clinical trials investigating medications for ASD and presenting both dichotomous and continuous CGI-I data were included. The number of patients with at least much improvement (CGI-I ≤ 2) were imputed from the CGI-I scale, assuming an underlying normal distribution of a latent continuous score using a primary threshold θ = 2.5 instead of θ = 2, which is the original cut-off in the CGI-I scale. The original and imputed values were used to calculate responder rates and odds ratios. The performance of the imputation method was investigated with a concordance correlation coefficient (CCC), linear regression, Bland-Altman plots, and subgroup differences of summary estimates obtained from random-effects meta-analysis.
Data from 27 studies, 58 arms, and 1428 participants were used. The imputation method using the primary threshold (θ = 2.5) had good performance for the responder rates (CCC = 0.93 95% confidence intervals [0.86, 0.96]; β of linear regression = 1.04 [0.95, 1.13]; bias and limits of agreements = 4.32% [-8.1%, 16.74%]; no subgroup differences χ = 1.24, -value = 0.266) and odds ratios (CCC = 0.91 [0.86, 0.96]; β = 0.96 [0.78, 1.14]; bias = 0.09 [-0.87, 1.04]; χ = 0.02, -value = 0.894). The imputation method had poorer performance when the secondary threshold (θ = 2) was used.
Assuming a normal distribution of the CGI-I scale, the number of responders could be imputed from the mean and standard deviation and used in meta-analysis. Due to the wide limits of agreement of the imputation method, sensitivity analysis excluding studies with imputed values should be performed.
在自闭症谱系障碍(ASD)的临床试验中,根据临床总体印象改善量表(CGI-I)评估的治疗反应是一种易于解释的结果。然而,CGI-I评分有时被报告为连续结果,将其转换为二分法可使荟萃分析纳入更多证据。
纳入了调查用于治疗ASD的药物并同时呈现二分法和连续CGI-I数据的临床试验。从CGI-I量表中推算出至少有明显改善(CGI-I≤2)的患者数量,假设潜在连续评分呈正态分布,使用的主要阈值θ = 2.5而非CGI-I量表中的原始临界值θ = 2。使用原始值和推算值来计算缓解率和比值比。通过一致性相关系数(CCC)、线性回归、布兰德-奥特曼图以及随机效应荟萃分析得出的汇总估计值的亚组差异来研究推算方法的性能。
使用了来自27项研究、58个治疗组和1428名参与者的数据。使用主要阈值(θ = 2.5)的推算方法在缓解率方面表现良好(CCC = 0.93,95%置信区间[0.86, 0.96];线性回归的β = 1.04 [0.95, 1.13];偏差和一致性界限 = 4.32% [-8.1%, 16.74%];无亚组差异,χ = 1.24,P值 = 0.266)以及比值比方面(CCC = 0.91 [0.86, 0.96];β = 0.96 [0.78, 1.14];偏差 = 0.09 [-0.87, 1.04];χ = 0.02,P值 = 0.894)。当使用次要阈值(θ = 2)时,推算方法的性能较差。
假设CGI-I量表呈正态分布,可从均值和标准差推算出缓解者数量并用于荟萃分析。由于推算方法的一致性界限较宽,应进行敏感性分析,排除使用推算值的研究。