Centre for Perinatal Neuroscience, Imperial College London, London, UK.
Centre for Perinatal Neuroscience, Imperial College London, London, UK.
Lancet Glob Health. 2021 Sep;9(9):e1273-e1285. doi: 10.1016/S2214-109X(21)00264-3. Epub 2021 Aug 3.
Although therapeutic hypothermia reduces death or disability after neonatal encephalopathy in high-income countries, its safety and efficacy in low-income and middle-income countries is unclear. We aimed to examine whether therapeutic hypothermia alongside optimal supportive intensive care reduces death or moderate or severe disability after neonatal encephalopathy in south Asia.
We did a multicountry open-label, randomised controlled trial in seven tertiary neonatal intensive care units in India, Sri Lanka, and Bangladesh. We enrolled infants born at or after 36 weeks of gestation with moderate or severe neonatal encephalopathy and a need for continued resuscitation at 5 min of age or an Apgar score of less than 6 at 5 min of age (for babies born in a hospital), or both, or an absence of crying by 5 min of age (for babies born at home). Using a web-based randomisation system, we allocated infants into a group receiving whole body hypothermia (33·5°C) for 72 h using a servo-controlled cooling device, or to usual care (control group), within 6 h of birth. All recruiting sites had facilities for invasive ventilation, cardiovascular support, and access to 3 Tesla MRI scanners and spectroscopy. Masking of the intervention was not possible, but those involved in the magnetic resonance biomarker analysis and neurodevelopmental outcome assessments were masked to the allocation. The primary outcome was a combined endpoint of death or moderate or severe disability at 18-22 months, assessed by the Bayley Scales of Infant and Toddler Development (third edition) and a detailed neurological examination. Analysis was by intention to treat. This trial is registered with ClinicalTrials.gov, NCT02387385.
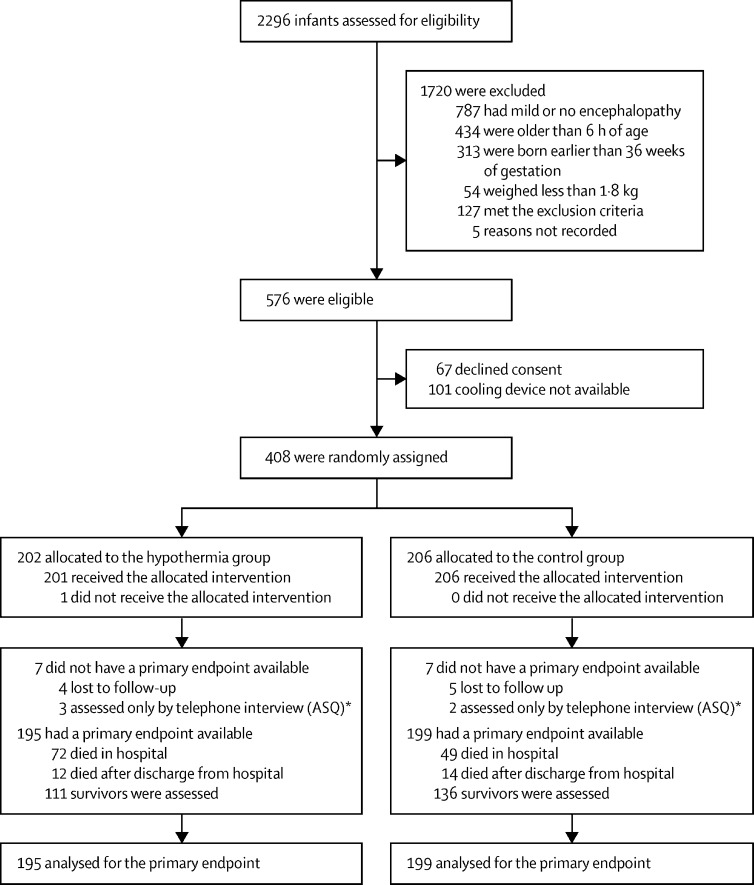
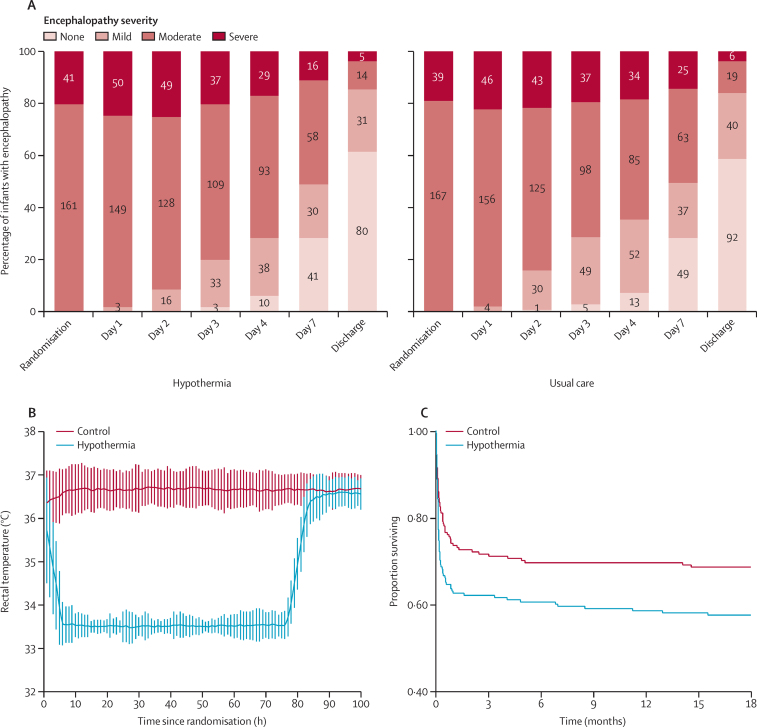
We screened 2296 infants between Aug 15, 2015, and Feb 15, 2019, of whom 576 infants were eligible for inclusion. After exclusions, we recruited 408 eligible infants and we assigned 202 to the hypothermia group and 206 to the control group. Primary outcome data were available for 195 (97%) of the 202 infants in the hypothermia group and 199 (97%) of the 206 control group infants. 98 (50%) infants in the hypothermia group and 94 (47%) infants in the control group died or had a moderate or severe disability (risk ratio 1·06; 95% CI 0·87-1·30; p=0·55). 84 infants (42%) in the hypothermia group and 63 (31%; p=0·022) infants in the control group died, of whom 72 (36%) and 49 (24%; p=0·0087) died during neonatal hospitalisation. Five serious adverse events were reported: three in the hypothermia group (one hospital readmission relating to pneumonia, one septic arthritis, and one suspected venous thrombosis), and two in the control group (one related to desaturations during MRI and other because of endotracheal tube displacement during transport for MRI). No adverse events were considered causally related to the study intervention.
Therapeutic hypothermia did not reduce the combined outcome of death or disability at 18 months after neonatal encephalopathy in low-income and middle-income countries, but significantly increased death alone. Therapeutic hypothermia should not be offered as treatment for neonatal encephalopathy in low-income and middle-income countries, even when tertiary neonatal intensive care facilities are available.
National Institute for Health Research, Garfield Weston Foundation, and Bill & Melinda Gates Foundation.
For the Hindi, Malayalam, Telugu, Kannada, Singhalese, Tamil, Marathi and Bangla translations of the abstract see Supplementary Materials section.
尽管在高收入国家,治疗性低温可降低新生儿脑病后的死亡或残疾发生率,但在中低收入国家,其安全性和疗效尚不清楚。我们旨在研究在南亚,与最佳支持性强化护理联合使用的治疗性低温是否可降低新生儿脑病后的死亡或中重度残疾发生率。
我们在印度、斯里兰卡和孟加拉国的 7 个三级新生儿重症监护病房进行了一项多国家、开放性、随机对照试验。我们纳入了胎龄在 36 周及以上、需要在出生后 5 分钟时持续复苏或在 5 分钟时 Apgar 评分<6 的中度或重度新生儿脑病患儿(在医院出生的婴儿),或两者均需复苏的婴儿,或在出生后 5 分钟时无哭声的婴儿(在家中出生的婴儿)。我们使用基于网络的随机化系统,在出生后 6 小时内将婴儿分配到全身接受 33.5°C 的体温控制(使用伺服控制冷却设备)的低温组或接受常规护理(对照组)。不可能对干预措施进行盲法,但参与磁共振生物标志物分析和神经发育结局评估的人员对分配情况不知情。
主要结局是在 18-22 个月时采用贝利婴幼儿发育量表(第三版)和详细的神经检查评估的死亡或中重度残疾的联合终点。分析采用意向治疗。本试验在 ClinicalTrials.gov 上注册,编号为 NCT02387385。
我们于 2015 年 8 月 15 日至 2019 年 2 月 15 日期间筛查了 2296 名婴儿,其中 576 名婴儿符合纳入条件。排除后,我们纳入了 408 名符合条件的婴儿,将 202 名婴儿分配到低温组,206 名婴儿分配到对照组。低温组的 202 名婴儿和对照组的 206 名婴儿中,195 名(97%)和 199 名(97%)有主要结局数据。低温组 98 名(50%)婴儿和对照组 94 名(47%)婴儿死亡或存在中重度残疾(风险比 1.06;95%CI 0.87-1.30;p=0.55)。低温组 84 名(42%)婴儿和对照组 63 名(31%)婴儿死亡(p=0.022),其中 72 名(36%)和 49 名(24%)婴儿在新生儿住院期间死亡(p=0.0087)。报告了 5 例严重不良事件:低温组 3 例(1 例与肺炎相关的再次住院,1 例脓毒性关节炎,1 例疑似静脉血栓形成),对照组 2 例(1 例与 MRI 期间的饱和度下降有关,另 1 例与 MRI 转运时气管插管移位有关)。没有不良事件被认为与研究干预有因果关系。
在中低收入国家,治疗性低温并未降低新生儿脑病后 18 个月时的死亡或残疾联合结局,但显著增加了单独的死亡率。即使有三级新生儿重症监护病房,也不应将治疗性低温作为中低收入国家新生儿脑病的治疗方法。
英国国家卫生研究院、加菲尔德·韦斯顿基金会和比尔及梅琳达·盖茨基金会。