Siemert Julia, Wald Theresa, Kolb Marlen, Pettinella Isolde, Böhm Ulrike, Pirlich Markus, Wiegand Susanne, Dietz Andreas, Wichmann Gunnar
Department of Otorhinolaryngology, Head and Neck Surgery, University Hospital Leipzig, Liebigstr, 10-14, 04103 Leipzig, Germany.
Cancers (Basel). 2021 Jul 27;13(15):3781. doi: 10.3390/cancers13153781.
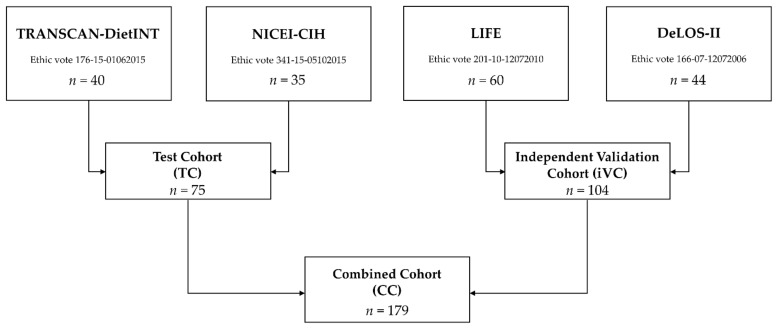
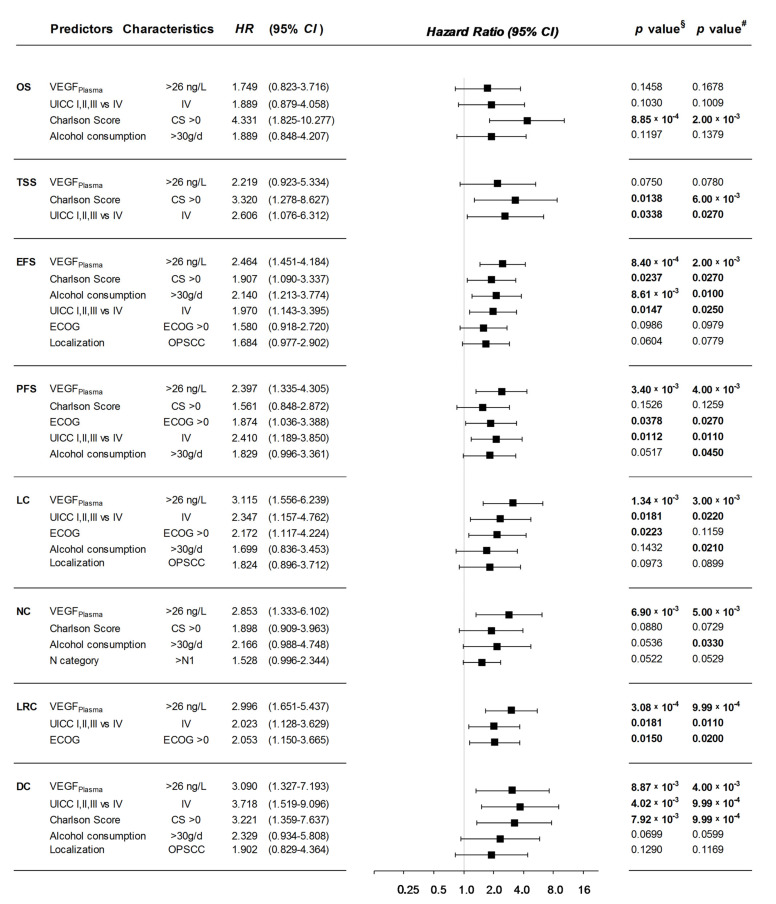
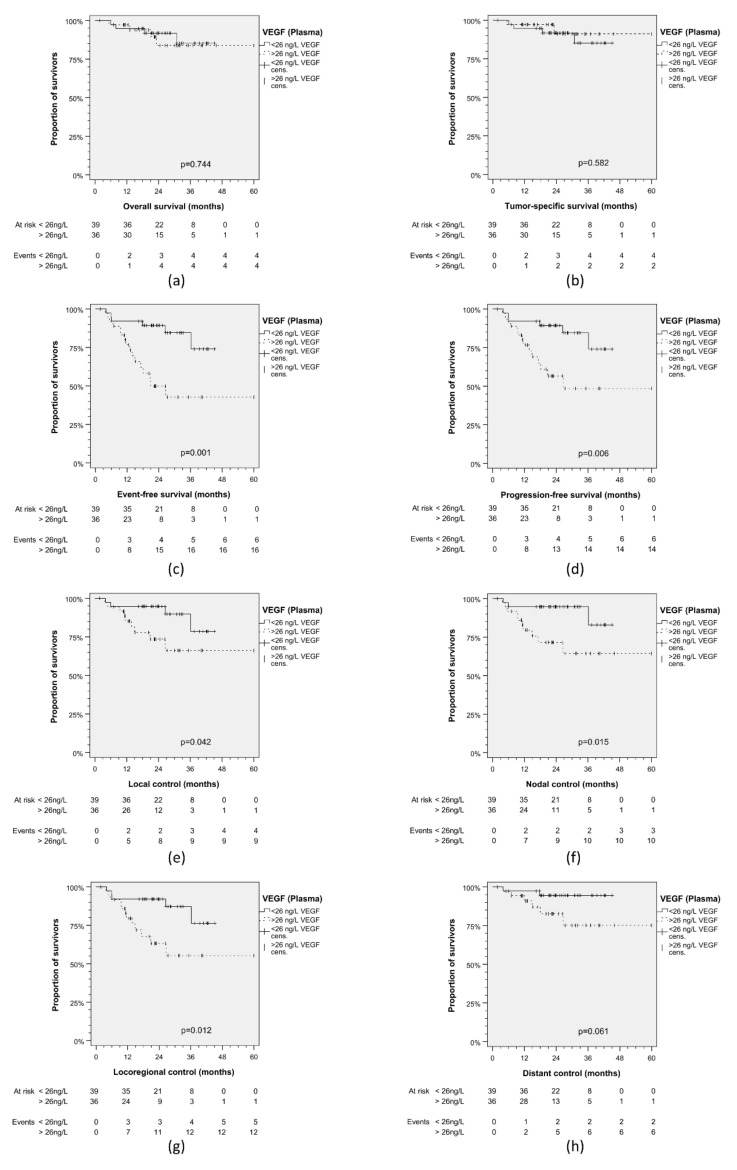
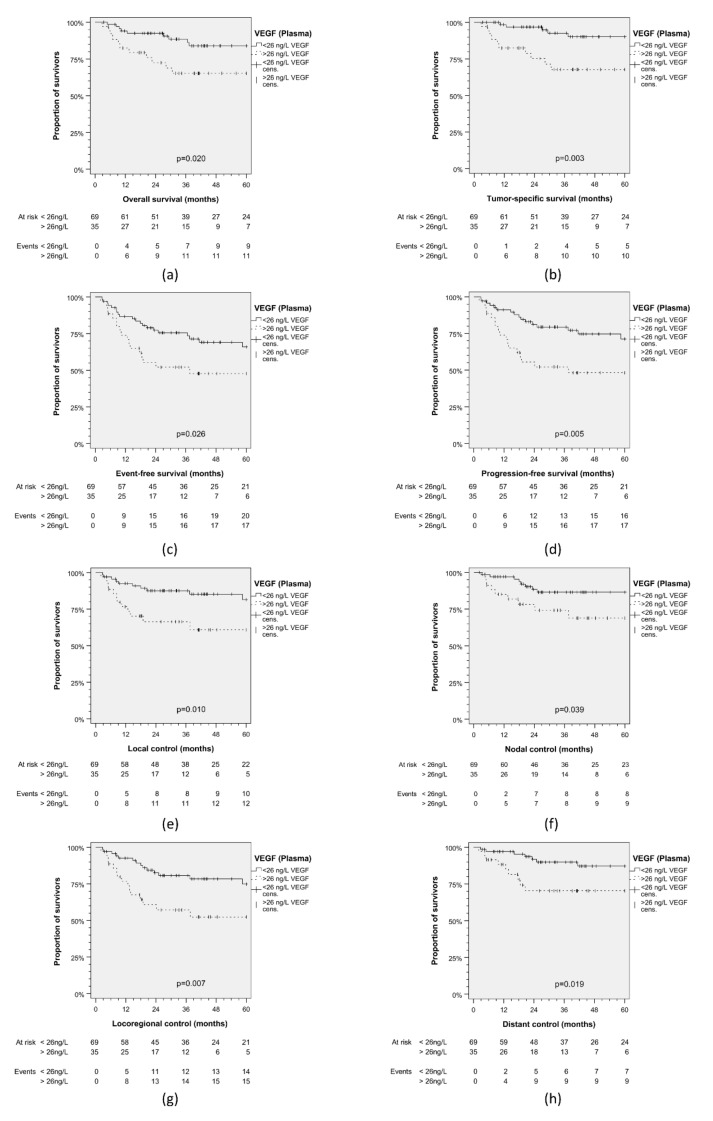
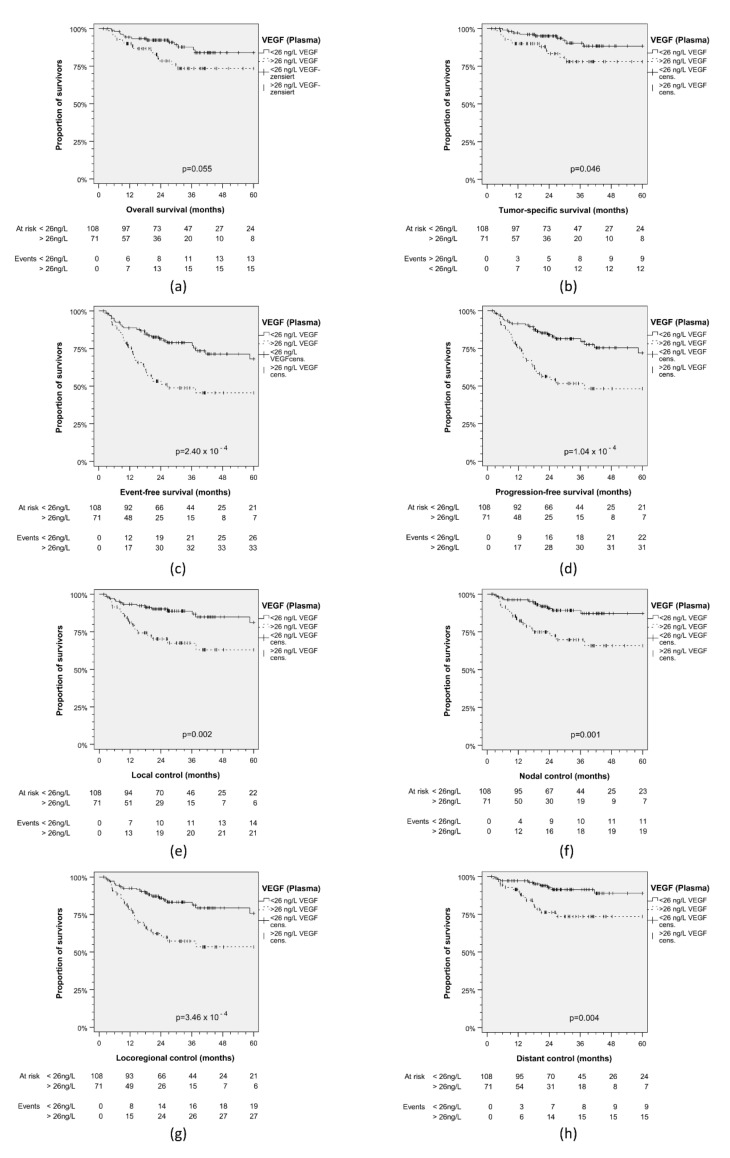
Vascular endothelial growth factor (VEGF) is centrally involved in cancer angiogenesis. We hypothesized that pre-therapeutic VEGF levels in serum and plasma differ in their potential as biomarkers for outcomes in head and neck squamous cell carcinoma (HNSCC) patients. As prospectively defined in the study protocols of TRANSCAN-DietINT and NICEI-CIH, we measured VEGF in pretreatment serum and plasma of 75 HNSCC test cohort (TC) patients. We analyzed the prognostic value of VEGF concentrations in serum (VEGF) and plasma (VEGF) for event-free survival (EFS) utilizing receiver-operating characteristics (ROC). Mean VEGF concentrations in plasma (34.6, 95% CI 26.0-43.3 ng/L) were significantly lower ( = 3.35 × 10) than in serum (214.8, 95% CI 179.6-250.0 ng/L) but, based on ROC (area under the curve, AUC = 0.707, 95% CI 0.573-0.840; = 0.006 versus AUC = 0.665, 95% CI 0.528-0.801; = 0.030), superiorly correlated with event-free survival (EFS) of TC patients. Youden indices revealed optimum binary classification with VEGF 26 ng/L and VEGF 264 ng/L. Kaplan-Meier plots demonstrated superiority of VEGF in discriminating patients regarding outcome. Patients with VEGF < 26 ng/L had superior nodal (NC), local (LC) and loco-regional control (LRC) leading to significant prolonged progression-free survival (PFS) and EFS. We successfully validated VEGF according the cut-off <26 ng/L as predictive for superior outcome in an independent validation cohort (iVC) of 104 HNSCC patients from the studies DeLOS-II and LIFE and found better outcomes including prolonged tumor-specific (TSS) and overall survival (OS). Outcomes in TC and iVC combined again was related to VEGF, and multivariate Cox regression revealed that VEGF was an independent outcome predictor. In HNSCC, pre-therapeutic VEGF is prognostic for outcomes.
血管内皮生长因子(VEGF)在癌症血管生成中起核心作用。我们假设,血清和血浆中的治疗前VEGF水平在作为头颈部鳞状细胞癌(HNSCC)患者预后生物标志物的潜力方面存在差异。按照TRANSCAN-DietINT和NICEI-CIH研究方案中的前瞻性定义,我们测量了75例HNSCC测试队列(TC)患者治疗前血清和血浆中的VEGF。我们利用受试者工作特征(ROC)分析了血清(VEGF)和血浆(VEGF)中VEGF浓度对无事件生存期(EFS)的预后价值。血浆中的平均VEGF浓度(34.6,95%CI 26.0 - 43.3 ng/L)显著低于血清中的浓度(214.8,95%CI 179.6 - 250.0 ng/L)(P = 3.35×10),但基于ROC分析(曲线下面积,AUC = 0.707,95%CI 0.573 - 0.840;P = 0.006,而血清AUC = 0.665,95%CI 0.528 - 0.801;P = 0.030),血浆VEGF与TC患者的无事件生存期(EFS)具有更好的相关性。约登指数显示,VEGF为26 ng/L和VEGF为264 ng/L时二元分类最佳。Kaplan-Meier曲线表明VEGF在区分患者预后方面具有优势。VEGF < 26 ng/L的患者在淋巴结(NC)、局部(LC)和局部区域控制(LRC)方面表现更佳,从而显著延长了无进展生存期(PFS)和无事件生存期(EFS)。我们在来自DeLOS-II和LIFE研究的104例HNSCC患者的独立验证队列(iVC)中成功验证了VEGF < 26 ng/L的临界值可预测更好的预后,并发现包括延长肿瘤特异性生存期(TSS)和总生存期(OS)在内的更好结局。TC和iVC合并后的结局再次与VEGF相关,多因素Cox回归显示VEGF是一个独立的结局预测因子。在HNSCC中,治疗前VEGF可预测预后。