College & Hospital of Stomatology, Key Lab. of Oral Diseases Research of Anhui Province, Anhui Medical University, Hefei, China.
The First Affiliated Hospital (First Clinical Medical College), Anhui Medical University, Hefei, China.
J Cancer Res Clin Oncol. 2024 Feb 12;150(2):91. doi: 10.1007/s00432-024-05606-8.
To develop a model that can assist in the diagnosis and prediction of prognosis for head and neck squamous cell carcinoma (HNSCC).
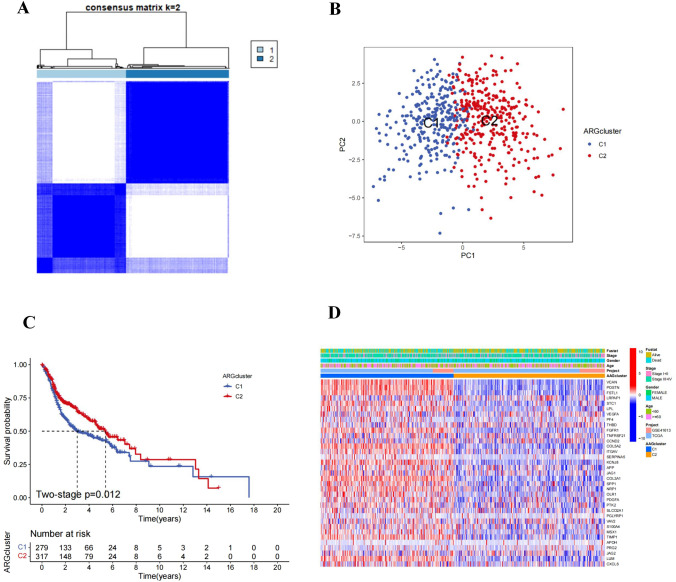
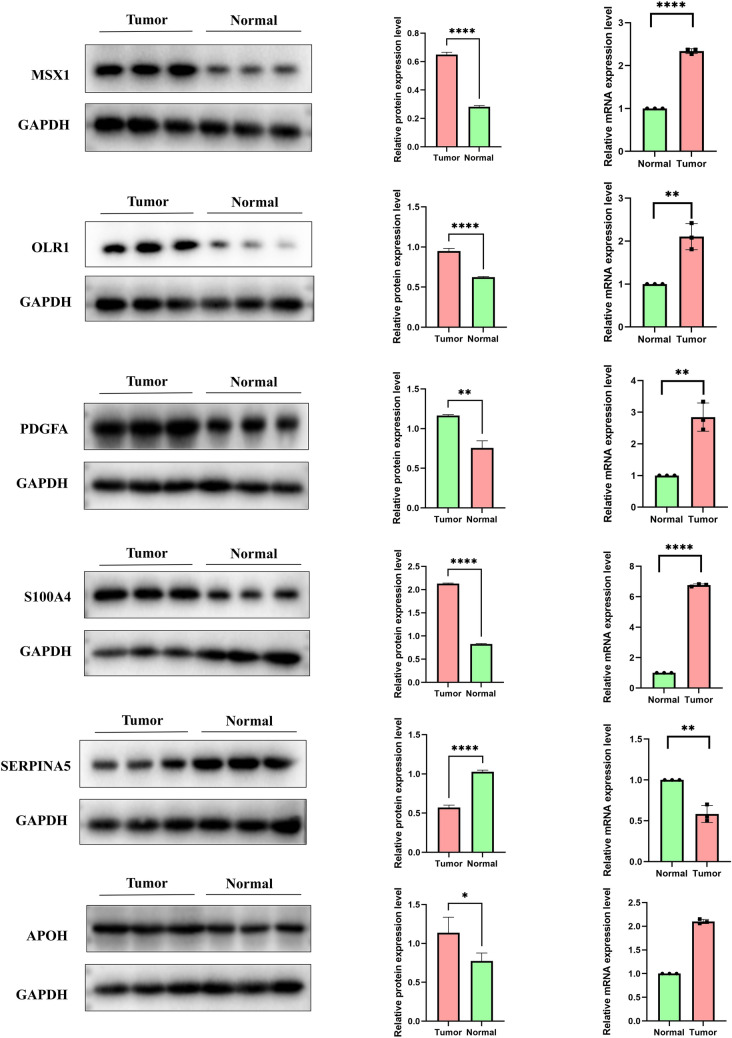
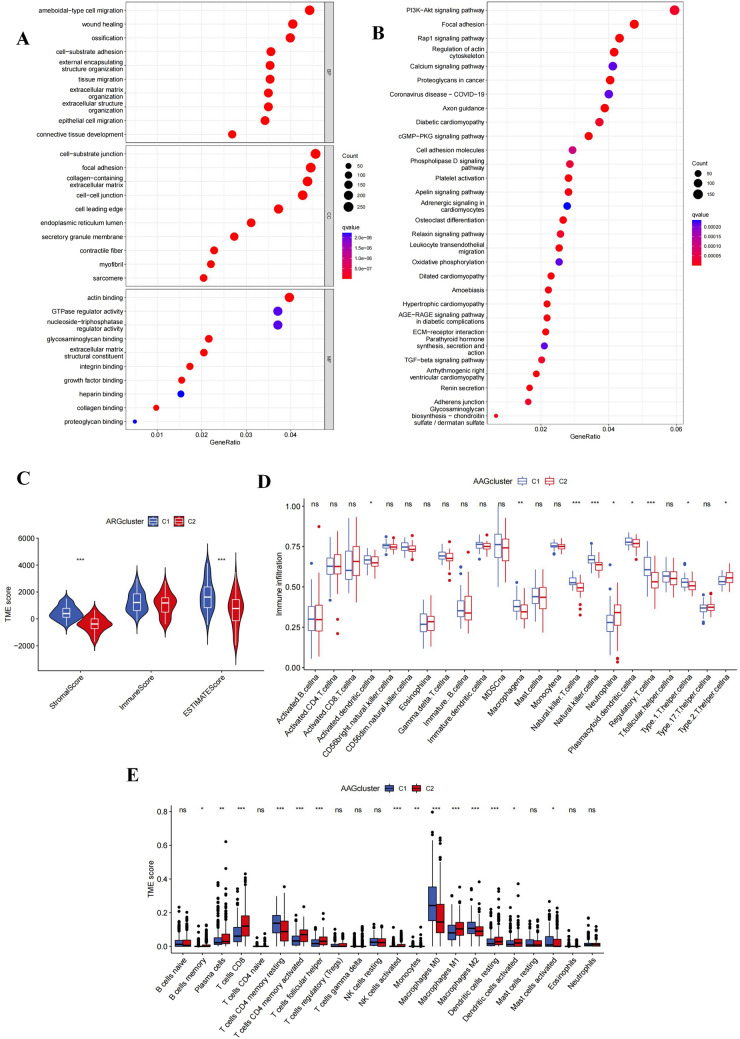
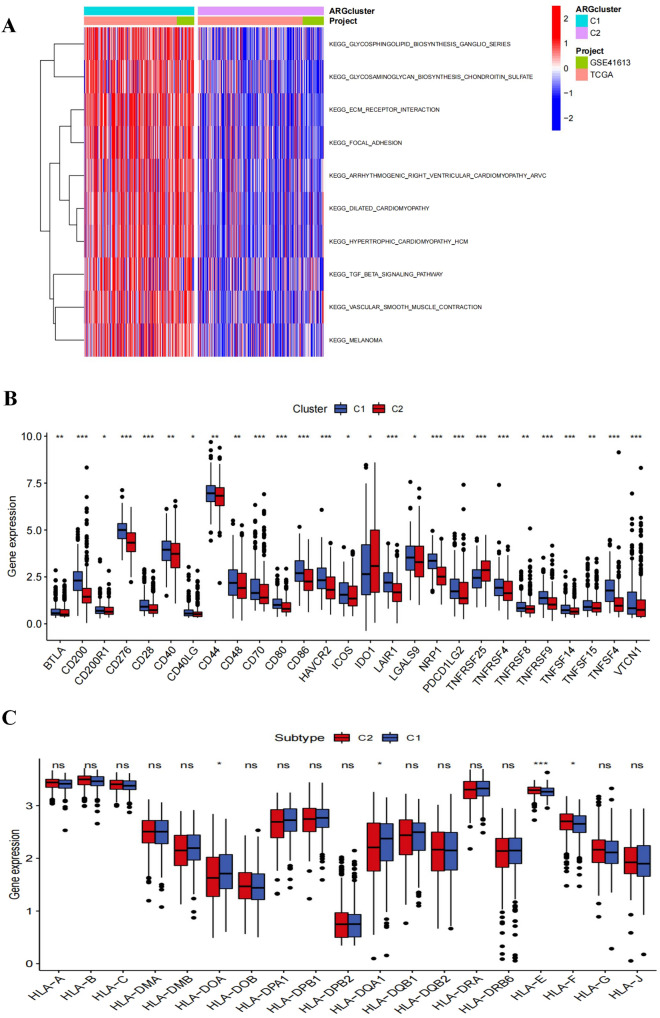
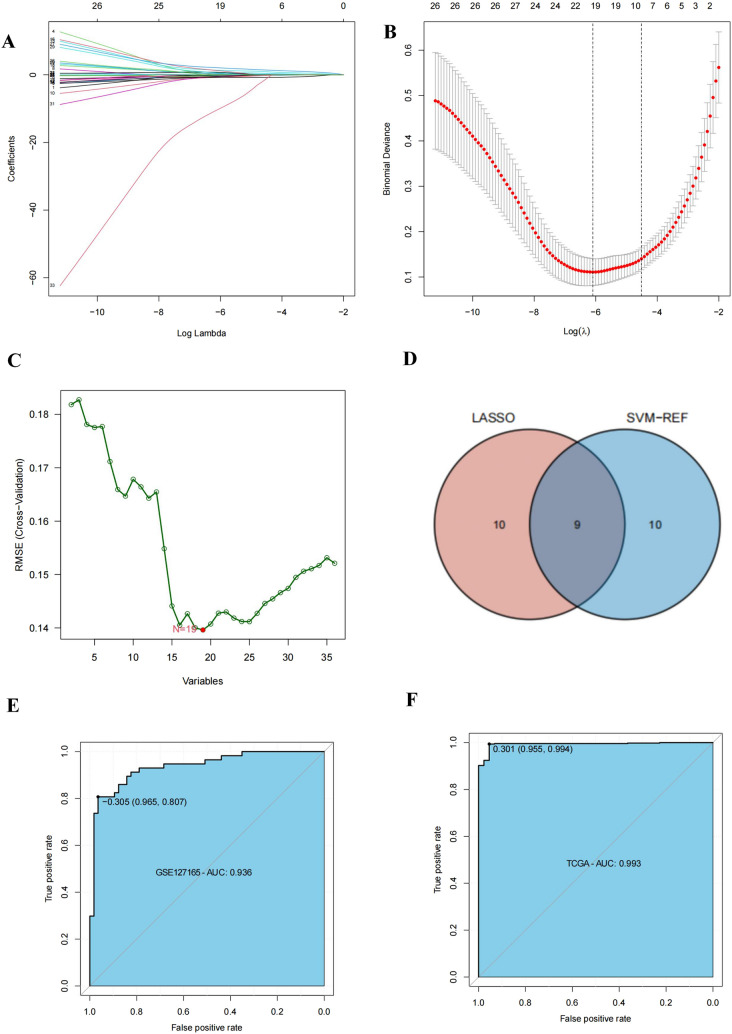
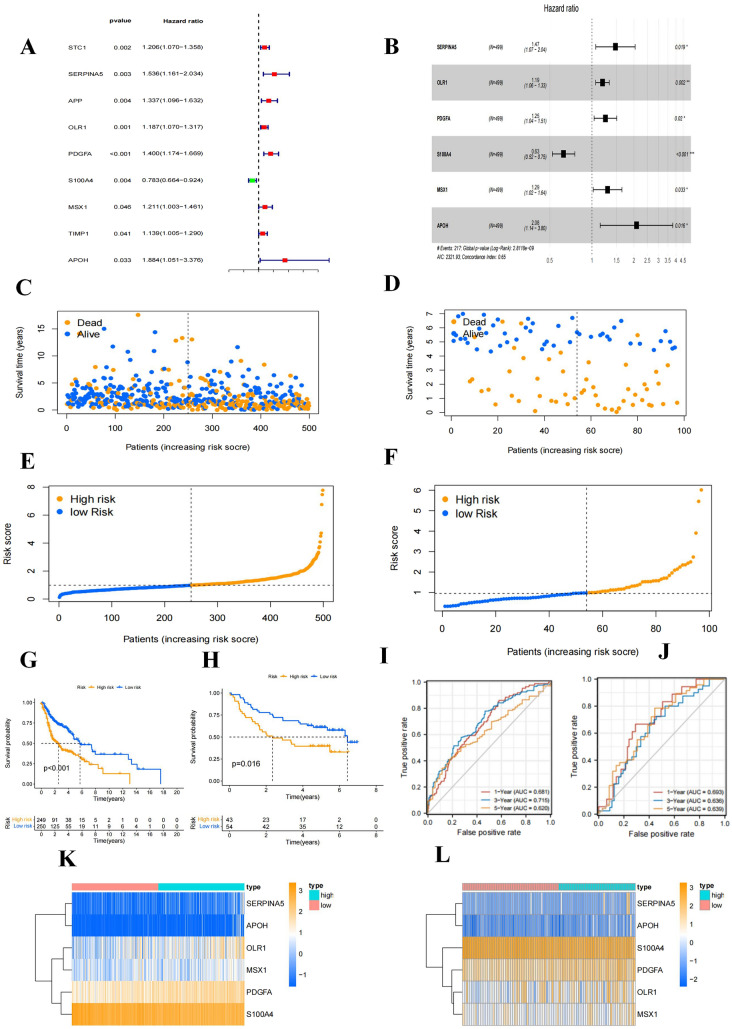
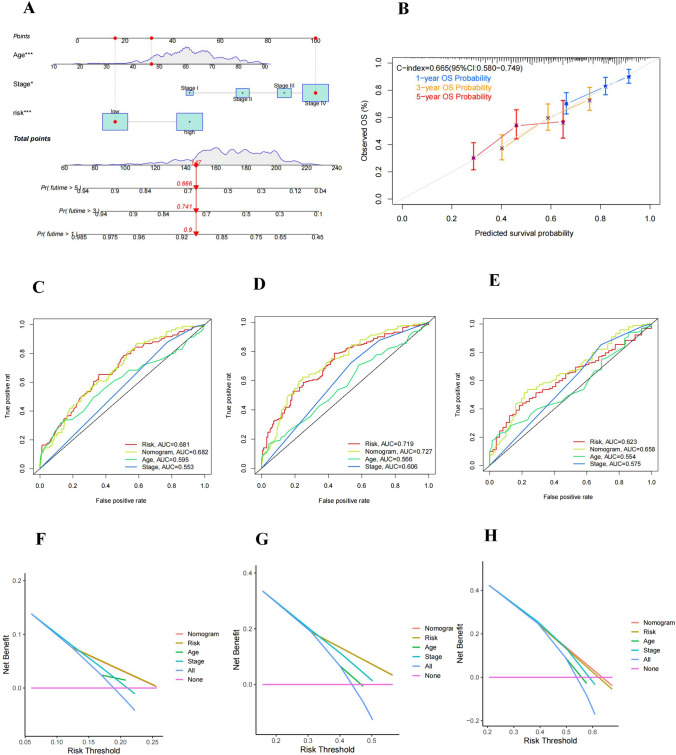
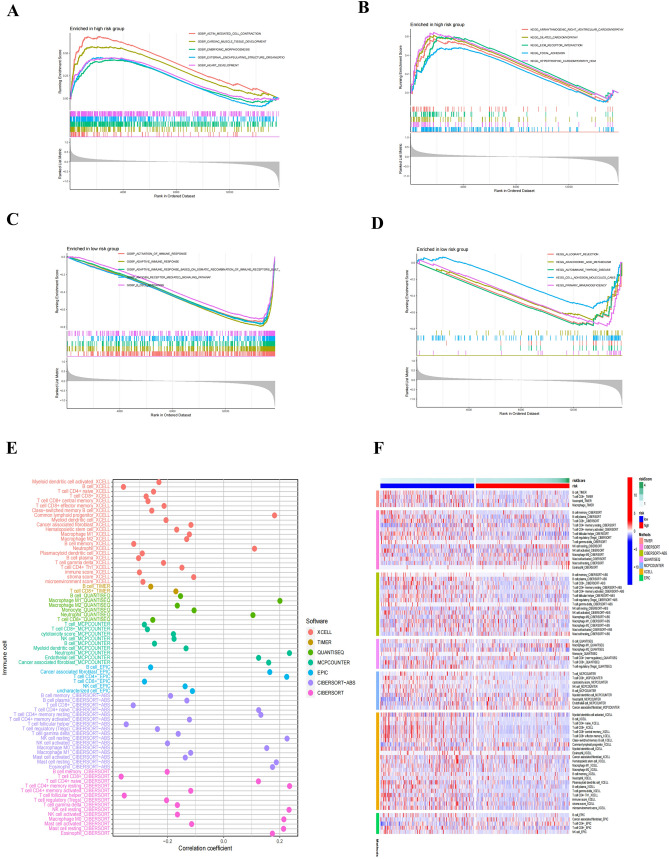
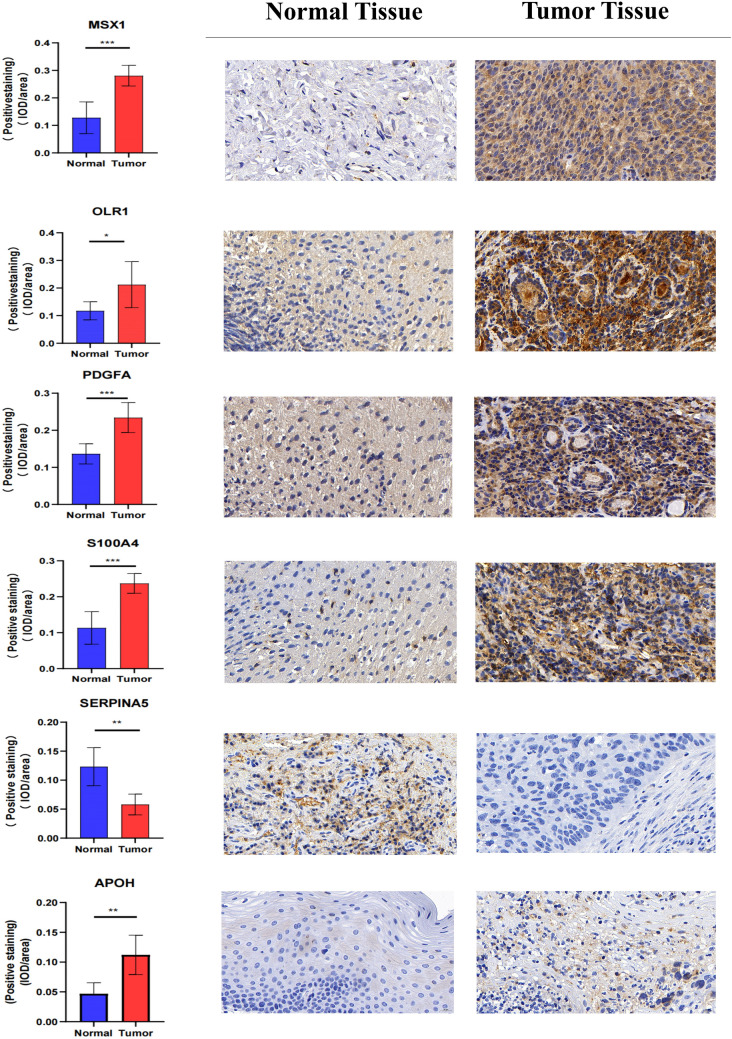
Data from TCGA and GEO databases were used to generate normalized gene expression data. Consensus Cluster Plus was used for cluster analysis and the relationship between angiogenesis-associated gene (AAG) expression patterns, clinical characteristics and survival was examined. Support vector machine (SVM) and least absolute shrinkage and selection operator (LASSO) analyzes and multiple logistic regression analyzes were performed to determine the diagnostic model, and a prognostic nomogram was constructed using univariate and multivariate Cox regression analyses. ESTIMATE, XCELL, TIMER, QUANTISEQ, MCPCOUNTER, EPIC, CIBERSORT-ABS, CIBERSORT algorithms were used to assess the immune microenvironment of HNSCC patients. In addition, gene set enrichment analysis, treatment sensitivity analysis, and AAGs mutation studies were performed. Finally, we also performed immunohistochemistry (IHC) staining in the tissue samples.
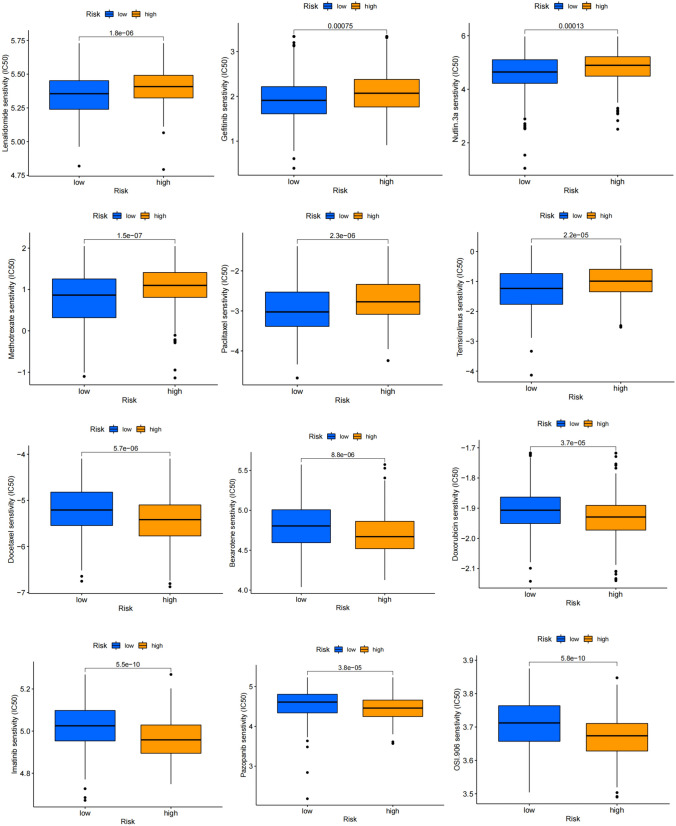
We classified HNSCC patients into subtypes based on differences in AAG expression from TCGA and GEO databases. There are differences in clinical features, TME, and immune-related gene expression between two subgroups. We constructed a HNSCC diagnostic model based on nine AAGs, which has good sensitivity and specificity. After further screening, we constructed a prognostic risk signature for HNSCC based on six AAGs. The constructed risk score had a good independent prognostic significance, and it was further constructed into a prognostic nomogram together with age and stage. Different prognostic risk groups have differences in immune microenvironment, drug sensitivity, gene enrichment and gene mutation.
We have constructed a diagnostic and prognostic model for HNSCC based on AAG, which has good performance. The constructed prognostic risk score is closely related to tumor immune microenvironment and immunotherapy response.
开发一种能够辅助头颈部鳞状细胞癌(HNSCC)诊断和预测预后的模型。
利用 TCGA 和 GEO 数据库的数据生成标准化基因表达数据。采用 Consensus Cluster Plus 进行聚类分析,研究血管生成相关基因(AAG)表达模式与临床特征和生存之间的关系。采用支持向量机(SVM)和最小绝对收缩和选择算子(LASSO)分析以及多因素逻辑回归分析确定诊断模型,并通过单因素和多因素 Cox 回归分析构建预后列线图。采用 ESTIMATE、XCELL、TIMER、QUANTISEQ、MCPCOUNTER、EPIC、CIBERSORT-ABS、CIBERSORT 算法评估 HNSCC 患者的免疫微环境。此外,还进行了基因集富集分析、治疗敏感性分析和 AAG 突变研究。最后,我们还在组织样本中进行了免疫组织化学(IHC)染色。
我们根据 TCGA 和 GEO 数据库中 AAG 表达的差异将 HNSCC 患者分为不同亚型。两个亚组之间的临床特征、TME 和免疫相关基因表达存在差异。我们基于 9 个 AAG 构建了一个 HNSCC 诊断模型,该模型具有良好的敏感性和特异性。进一步筛选后,我们基于 6 个 AAG 构建了 HNSCC 预后风险特征。构建的风险评分具有良好的独立预后意义,并与年龄和分期一起进一步构建为预后列线图。不同的预后风险组在免疫微环境、药物敏感性、基因富集和基因突变方面存在差异。
我们基于 AAG 构建了 HNSCC 的诊断和预后模型,具有良好的性能。构建的预后风险评分与肿瘤免疫微环境和免疫治疗反应密切相关。