Laboratory of Clinical Immunology and Microbiology, NIAID, NIH, Bethesda, Md.
Division of Allergy, Immunology and Blood and Marrow Transplantation, Department of Pediatrics, University of California San Francisco School of Medicine, San Francisco, Calif; Smith Cardiovascular Research Institute, San Francisco, Calif; UCSF Benioff Children's Hospital, San Francisco, Calif.
J Allergy Clin Immunol. 2022 Mar;149(3):1113-1119. doi: 10.1016/j.jaci.2021.07.029. Epub 2021 Aug 9.
Development of a diverse T-cell receptor β (TRB) repertoire is associated with immune recovery following hematopoietic cell transplantation (HCT) for severe combined immunodeficiency (SCID). High-throughput sequencing of the TRB repertoire allows evaluation of clonotype dynamics during immune reconstitution.
We investigated whether longitudinal analysis of the TRB repertoire would accurately describe T-cell receptor diversity and illustrate the quality of T-cell reconstitution following HCT or gene therapy for SCID.
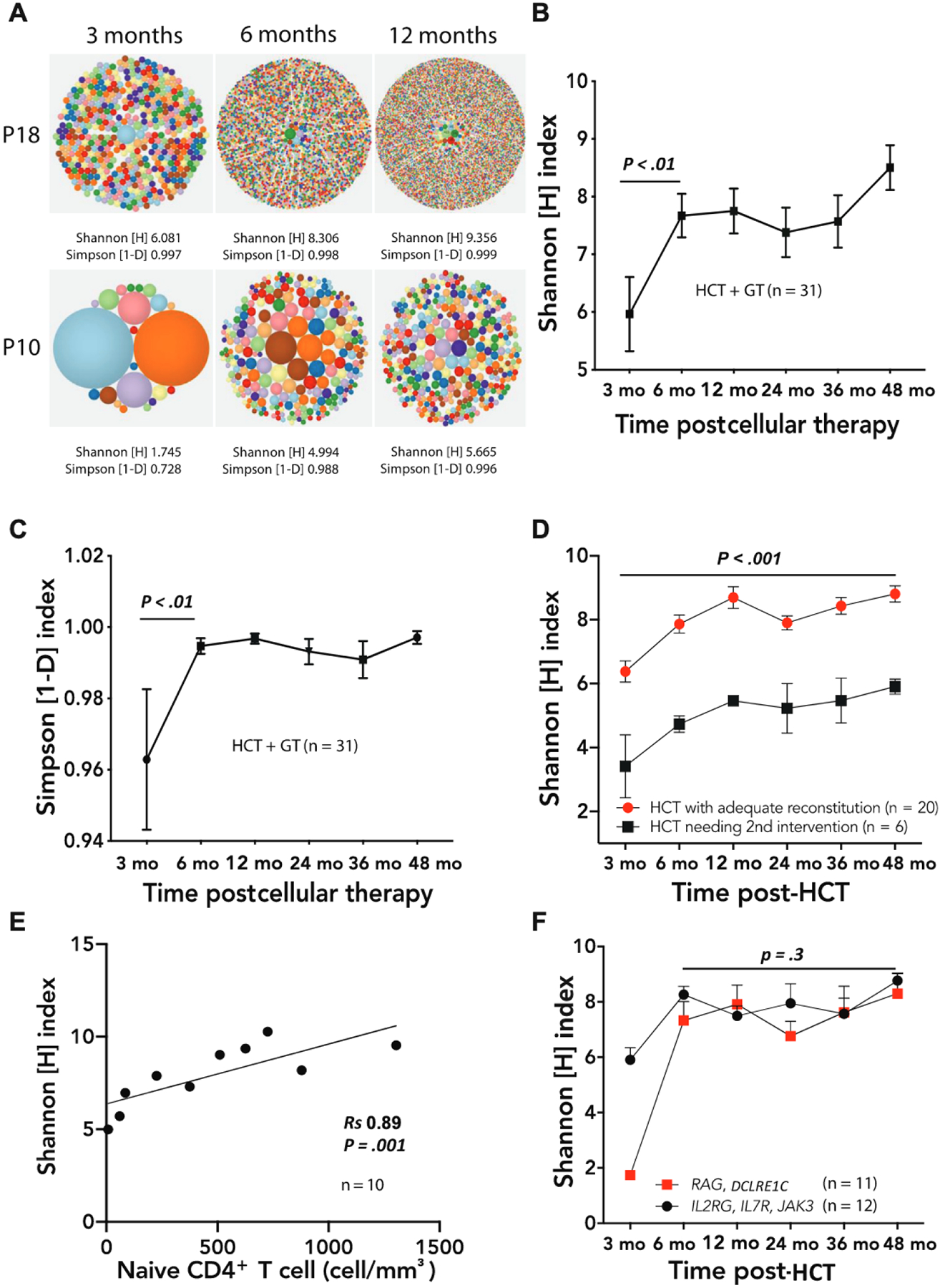
We used high-throughput sequencing to study composition and diversity of the TRB repertoire in 27 infants with SCID at 3, 6, and 12 months and yearly posttreatment(s). Total RNA from peripheral blood was used as template to amplify TRB rearrangements.
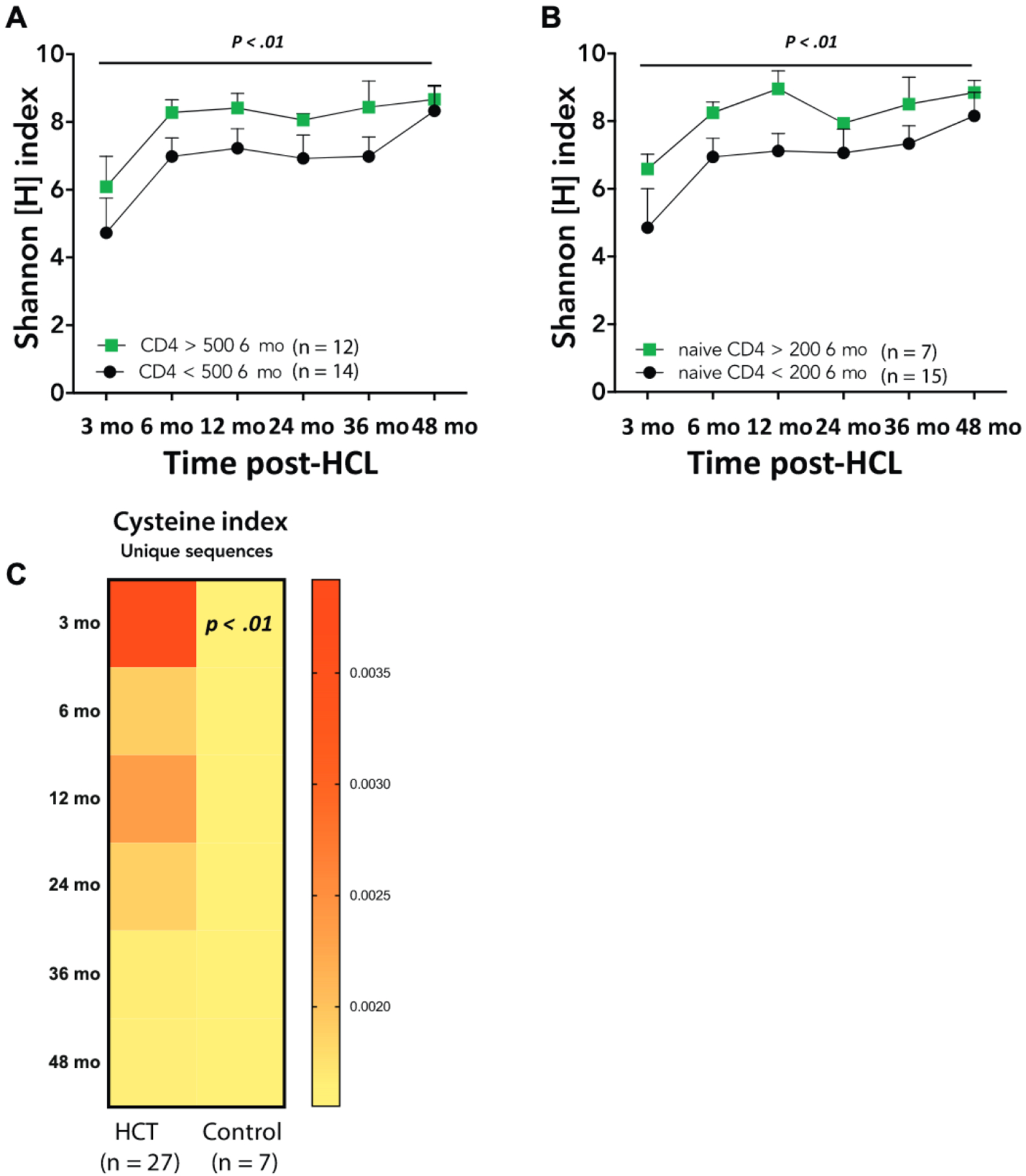
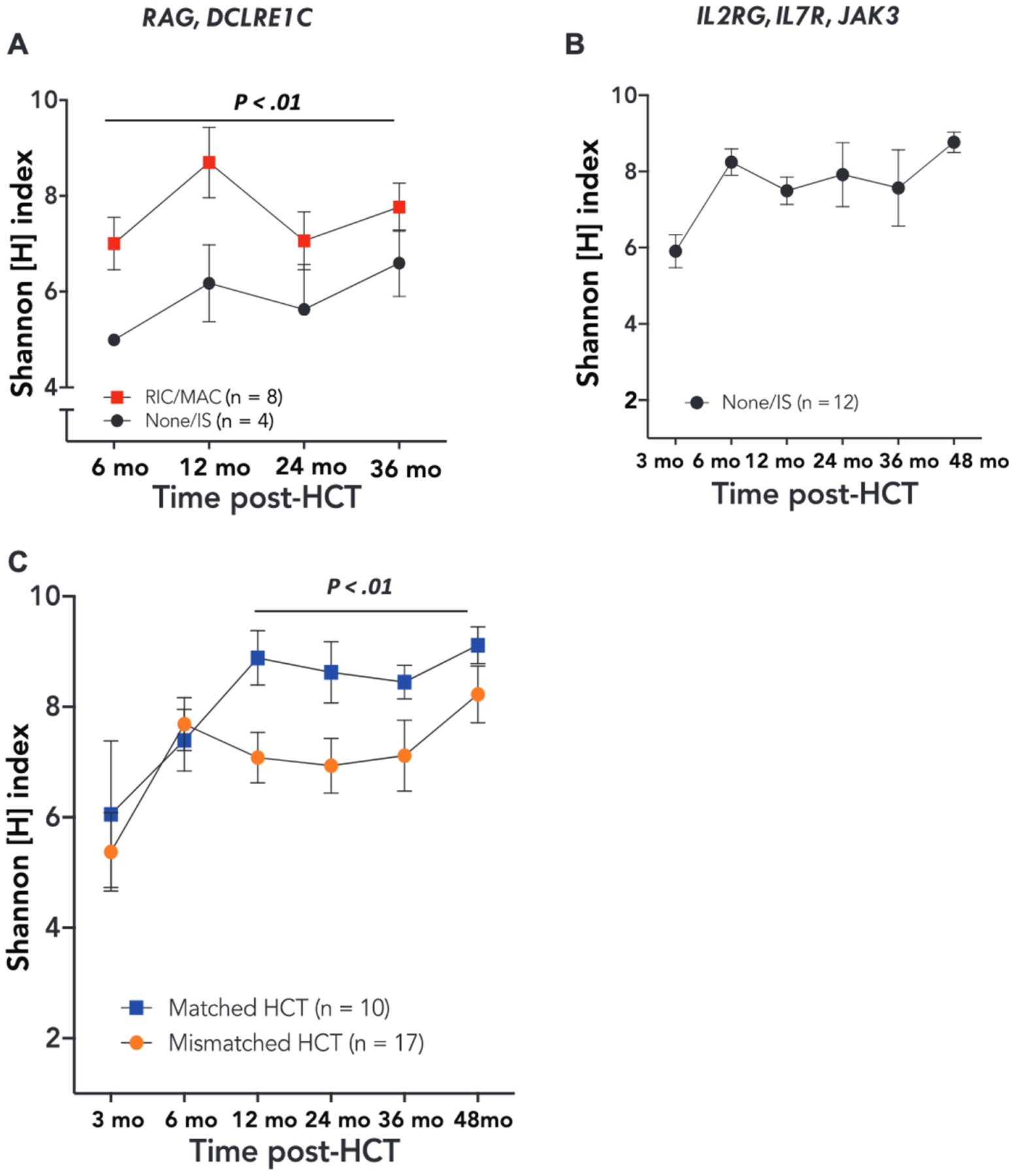
TRB sequence analysis showed poor diversity at 3 months, followed by significant improvement by 6 months after cellular therapies. Kinetics of development of TRB diversity were similar in patients with a range of underlying gene defects. However, in patients with RAG and DCLRE1C defects, HCT with no conditioning or immune suppression only resulted in lower diversity than did HCT with conditioning. HCT from a matched donor correlated with higher diversity than did HCT from a mismatched donor. Naive CD4 T-cell count at 6 months post-HCT correlated with higher TRB diversity. A Shannon index of diversity of 5.2 or lower 3 months after HCT predicted a need for a second intervention.
TRB repertoire after hematopoietic cell therapies for SCID provides a quantitative and qualitative measure of diversity of T-cell reconstitution and permits early identification of patients who may require a second intervention.
在接受造血细胞移植(HCT)治疗严重联合免疫缺陷(SCID)后,多样化的 T 细胞受体β(TRB)谱系的发展与免疫恢复相关。TRB 谱系的高通量测序可评估免疫重建过程中克隆型动态。
我们研究了 TRB 谱系的纵向分析是否能准确描述 T 细胞受体多样性,并说明 HCT 或基因治疗 SCID 后的 T 细胞重建质量。
我们使用高通量测序技术,在 3、6 和 12 个月及治疗后每年,研究 27 例 SCID 婴儿的 TRB 谱系组成和多样性。外周血总 RNA 用作模板扩增 TRB 重排。
TRB 序列分析显示 3 个月时多样性较差,随后在细胞治疗后 6 个月时显著改善。具有不同潜在基因缺陷的患者,TRB 多样性发展的动力学相似。然而,在 RAG 和 DCLRE1C 缺陷的患者中,无预处理或免疫抑制的 HCT 仅导致多样性低于 HCT 加预处理。与匹配供体的 HCT 与不匹配供体的 HCT 相比,相关性更高。HCT 后 6 个月的幼稚 CD4 T 细胞计数与更高的 TRB 多样性相关。HCT 后 3 个月时,多样性 Shannon 指数为 5.2 或更低,预测需要进行第二次干预。
SCID 造血细胞治疗后的 TRB 谱系为 T 细胞重建的多样性提供了定量和定性的测量,并允许早期识别可能需要进行第二次干预的患者。