Ying Yingfen, Lu Xiaosheng, Zhang Huina, Arhin Samuel Kofi, Hou Xiaohong, Wang Zefan, Wu Han, Lu Jieqiang, Tang Yunbing
Department of Obstetrics and Gynecology, The Second Affiliated Hospital and Yuying Children's Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, China.
School of Allied Health Sciences, University of Cape Coast, PMB, Cape Coast, Ghana.
PeerJ. 2021 Jul 26;9:e11785. doi: 10.7717/peerj.11785. eCollection 2021.
This study's objectives were to compare the clinical, perinatal, and obstetrical outcomes of patients with different estradiol (E) levels in fresh single-blastocyst-transfer (SBT) cycles under an early follicular phase prolonged regimen on the day of trigger.
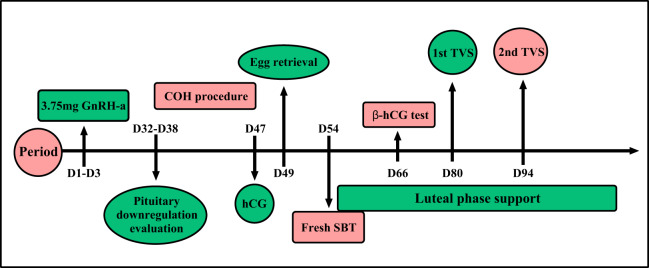
We recruited patients in fresh SBT cycles ( = 771) undergoing early follicular phase prolonged protocols with β-hCG values above 10 IU/L between June 2016 and December 2018. Patients who met the inclusion and exclusion criteria were divided into four groups according to their serum E level percentages on the day of trigger: <25, 25-50, 51-75, and >75 percentile groups.
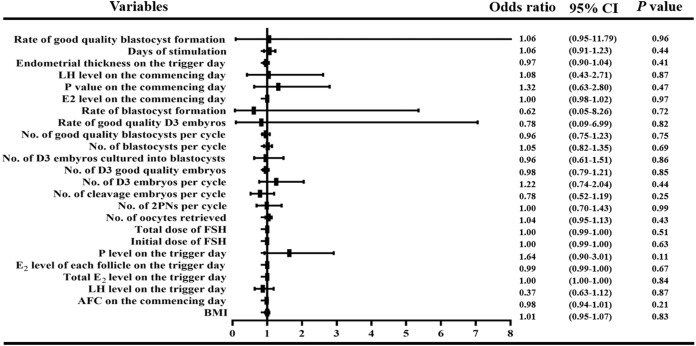
Although the rates of clinical pregnancy (85.57% (166/194)), embryo implantation 86.60% (168/194), ongoing pregnancy (71.13% (138/194)), and live birth (71.13% (138/194)) were lowest in the >75th percentile group, we did not observe any significant differences (all > 0.05). We used this information to predict the rate of severe ovarian hyperstimulation syndrome (OHSS) area under the curve (AUC) = 72.39%, = 0.029, cut off value of E = 2,893 pg/ml with the 75% sensitivity and 70% specificity. The 51-75 percentile group had the highest rates of low birth weight infants (11.73% (19/162), = 0.0408), premature delivery (11.43% (20/175), = 0.0269), admission to the neonatal intensive care unit (NICU) (10.49% (17/162), = 0.0029), twin pregnancies (8.57% (15/175), = 0.0047), and monochorionic diamniotic pregnancies (8.57% (15/175); = 0.001). We did not observe statistical differences in obstetrics complications, including gestational diabetes mellitus (GDM), gestational hypertension, placenta previa, premature rupture of membranes (PROM), and preterm premature rupture of membranes (PPROM).
We concluded that serum E levels on the day of trigger were not good predictors of live birth rate or perinatal and obstetrical outcomes. However, we found that high E levels may not be conducive to persistent pregnancies. The E level on the day of trigger can still be used to predict the incidence of early onset severe OHSS in the fresh SBT cycle.
本研究的目的是比较在卵泡期延长方案下,触发日进行新鲜单囊胚移植(SBT)周期时,不同雌二醇(E)水平患者的临床、围产期和产科结局。
我们招募了2016年6月至2018年12月期间接受卵泡期延长方案且β-hCG值高于10 IU/L的新鲜SBT周期患者(n = 771)。符合纳入和排除标准的患者根据触发日的血清E水平百分比分为四组:<25、25 - 50、51 - 75和>75百分位数组。
虽然>75百分位数组的临床妊娠率(85.57%(166/194))、胚胎着床率(86.60%(168/194))、持续妊娠率(71.13%(138/194))和活产率(71.13%(138/194))最低,但我们未观察到任何显著差异(均P>0.05)。我们利用这些信息预测重度卵巢过度刺激综合征(OHSS)的发生率,曲线下面积(AUC)= 72.39%,P = 0.029,E的截断值为2,893 pg/ml,敏感性为75%,特异性为70%。51 - 75百分位数组的低出生体重儿发生率最高(11.73%(19/162),P = 0.0408)、早产率(11.43%(20/175),P = 0.0269)、入住新生儿重症监护病房(NICU)率(10.49%(17/162),P = 0.0029)、双胎妊娠率(8.57%(15/175),P = 0.0047)和单绒毛膜双羊膜囊妊娠率(8.57%(15/175);P = 0.001)。我们未观察到包括妊娠期糖尿病(GDM)、妊娠期高血压、前置胎盘、胎膜早破(PROM)和早产胎膜早破(PPROM)在内的产科并发症的统计学差异。
我们得出结论,触发日的血清E水平不是活产率或围产期及产科结局的良好预测指标。然而,我们发现高E水平可能不利于持续妊娠。触发日的E水平仍可用于预测新鲜SBT周期中早发型重度OHSS的发生率。