Chitturi Kalyan R, Xu Jiaqiong, Araujo-Gutierrez Raquel, Bhimaraj Arvind, Guha Ashrith, Hussain Imad, Kassi Mahwash, Bernicker Eric H, Trachtenberg Barry H
Houston Methodist DeBakey Heart & Vascular Center, Houston, Texas, USA.
Center for Outcomes Research, Houston Methodist Research Institute, Houston, Texas, USA.
JACC CardioOncol. 2019 Dec 17;1(2):182-192. doi: 10.1016/j.jaccao.2019.11.013. eCollection 2019 Dec.
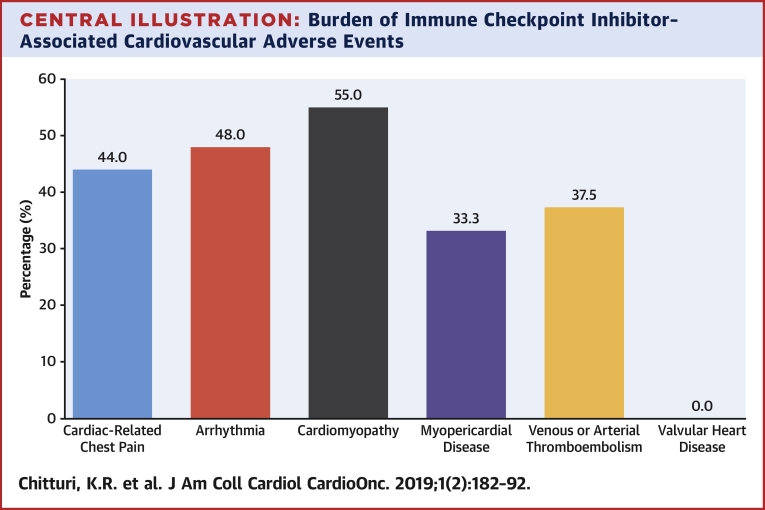
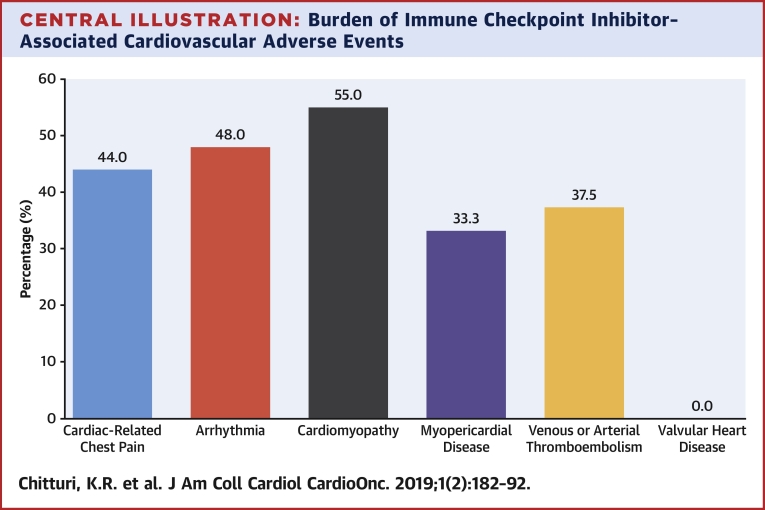
The purpose of this study was to evaluate whether immune checkpoint inhibitors (ICIs) are associated with an increased risk of major adverse cardiovascular events (MACE) compared with non-ICI therapies in patients with lung cancer.
ICIs activate the host immune system to target cancer cells. Though uncommon, cardiovascular immune-related adverse events can be life-threatening.
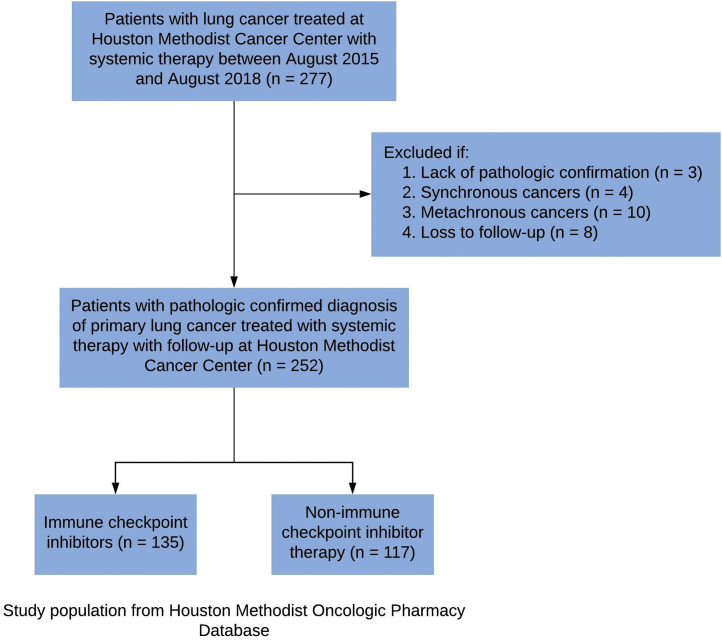
A retrospective single-institution cohort study of 252 patients with pathologically confirmed lung cancer who received ICI or non-ICI therapy was analyzed. The primary endpoint was MACE, defined as a composite of cardiovascular death, nonfatal myocardial infarction, nonfatal stroke, and hospitalization for heart failure.
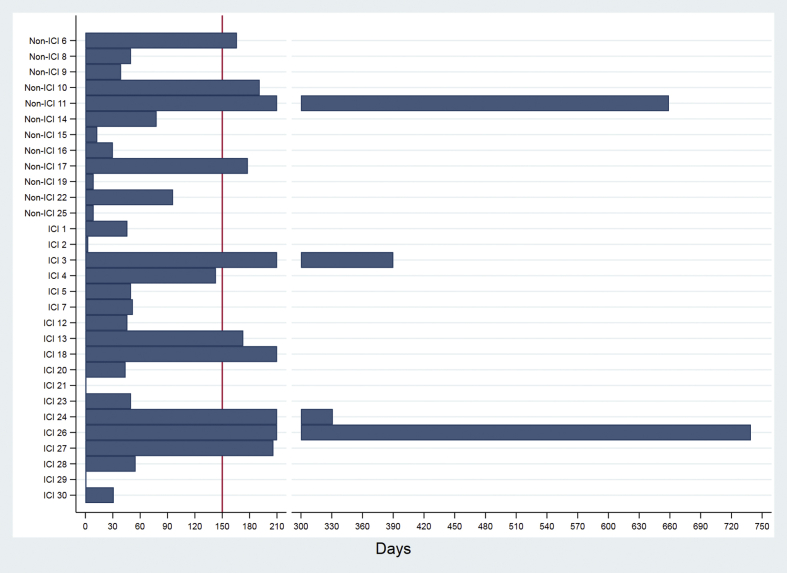
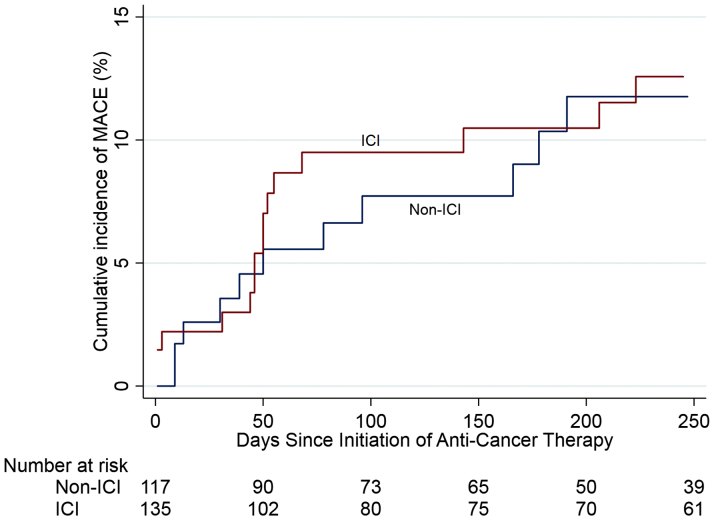
During a median follow-up of 6 months, MACE occurred in 13.3% of ICI-treated patients, with a median time to event of 51 days, compared with 10.3% and 64 days in non-ICI patients. ICIs were not associated with MACE (hazard ratio [HR]: 1.18; 95% confidence interval [CI]: 0.57 to 2.43; p = 0.66) in a univariable Fine-Gray regression analysis incorporating noncardiovascular death as a competing risk. Multivariable regression analyses determined that patients treated with ICIs with elevated serum troponin I >0.01 ng/ml (HR: 7.27; 95% CI: 2.72 to 19.43; p < 0.001) and B-type natriuretic peptide (BNP) >100 pg/ml (HR: 2.65; 95% CI: 1.01 to 6.92; p = 0.047) had an increased risk of MACE. Patients pre-treated or receiving combined immunotherapy with ICIs and vascular endothelial growth factor inhibitors (VEGFIs) or tyrosine kinase inhibitors (TKIs) had an increased risk of MACE (HR: 2.15; 95% CI: 1.05 to 4.37; p = 0.04).
ICIs were not independently associated with an increased risk of MACE in patients with lung cancer, although power is an important limitation in these analyses. ICI-associated cardiotoxicity was associated with elevations in serum troponin and BNP, and combined immunotherapy with VEGFIs or TKIs. Future studies are needed to further define the role of cardiac biomarkers as a monitoring strategy with ICI therapy.
本研究旨在评估与非免疫检查点抑制剂(ICI)疗法相比,免疫检查点抑制剂(ICI)是否会增加肺癌患者发生主要不良心血管事件(MACE)的风险。
ICI激活宿主免疫系统以靶向癌细胞。尽管不常见,但心血管免疫相关不良事件可能危及生命。
对252例经病理确诊的接受ICI或非ICI治疗的肺癌患者进行了一项回顾性单机构队列研究。主要终点是MACE,定义为心血管死亡、非致死性心肌梗死、非致死性卒中以及因心力衰竭住院的综合指标。
在中位随访6个月期间,接受ICI治疗的患者中有13.3%发生MACE,事件发生的中位时间为51天,相比之下,非ICI治疗患者的这一比例为10.3%,事件发生的中位时间为64天。在纳入非心血管死亡作为竞争风险的单变量Fine-Gray回归分析中,ICI与MACE无关(风险比[HR]:1.18;95%置信区间[CI]:0.57至2.43;p = 0.66)。多变量回归分析确定,血清肌钙蛋白I>0.01 ng/ml(HR:7.27;95% CI:2.72至19.43;p<0.001)和B型利钠肽(BNP)>100 pg/ml(HR:2.65;95% CI:1.01至6.92;p = 0.047)的ICI治疗患者发生MACE的风险增加。预先接受或接受ICI与血管内皮生长因子抑制剂(VEGFI)或酪氨酸激酶抑制剂(TKI)联合免疫治疗的患者发生MACE的风险增加(HR:2.15;95% CI:1.05至4.37;p = 0.04)。
ICI与肺癌患者发生MACE风险增加无独立相关性,尽管检验效能是这些分析中的一个重要局限。ICI相关心脏毒性与血清肌钙蛋白和BNP升高以及与VEGFI或TKI联合免疫治疗有关。未来需要进一步研究以明确心脏生物标志物作为ICI治疗监测策略的作用。