The University of Melbourne Department of Medicine, Melbourne Health and Northern Health, Royal Melbourne Hospital, Parkville, Victoria, Australia.
Kinghorn Centre for Clinical Genomics, Garvan Institute of Medical Research, Darlinghurst, New South Wales, Australia.
J Am Soc Nephrol. 2021 Sep;32(9):2273-2290. doi: 10.1681/ASN.2020071065. Epub 2021 Jun 18.
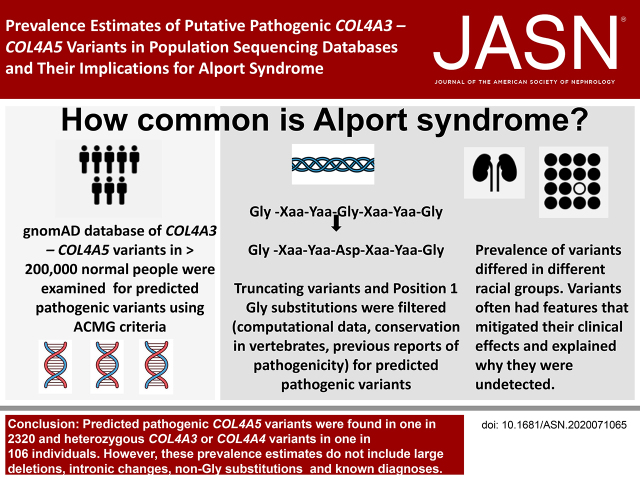
The reported prevalence of Alport syndrome varies from one in 5000 to one in 53,000 individuals. This study estimated the frequencies of predicted pathogenic variants in sequencing databases of populations without known kidney disease.
Predicted pathogenic variants were identified using filtering steps based on the ACMG/AMP criteria, which considered collagen IV 3-5 position 1 Gly to be critical domains. The population frequencies of predicted pathogenic variants were then determined per mean number of sequenced alleles. Population frequencies for compound heterozygous and digenic combinations were calculated from the results for heterozygous variants.
variants resulting in position 1 Gly substitutions were confirmed to be associated with hematuria (for each, <0.001). Predicted pathogenic variants were found in at least one in 2320 individuals. p.(Gly624Asp) represented nearly half (16 of 33, 48%) of the variants in Europeans. Most variants (54 of 59, 92%) had a biochemical feature that potentially mitigated the clinical effect. The predicted pathogenic heterozygous and variants affected one in 106 of the population, consistent with the finding of thin basement membrane nephropathy in normal donor kidney biopsy specimens. Predicted pathogenic compound heterozygous variants occurred in one in 88,866 individuals, and digenic variants in at least one in 44,793.
The population frequencies for Alport syndrome are suggested by the frequencies of predicted pathogenic variants, but must be adjusted for the disease penetrance of individual variants and for the likelihood of already diagnosed disease and non-Gly substitutions. Disease penetrance may depend on other genetic and environmental factors.
报道的 Alport 综合征患病率为每 5000 至每 53000 人中 1 例。本研究估计了无已知肾脏疾病人群的测序数据库中预测致病性变异的频率。
使用基于 ACMG/AMP 标准的过滤步骤识别预测致病性变异,该标准认为胶原蛋白 IV 3-5 位 1 甘氨酸为关键结构域。然后,根据平均测序等位基因数确定预测致病性变异的群体频率。杂合变体的结果计算出复合杂合子和双基因组合的群体频率。
导致 1 位甘氨酸取代的变异被证实与血尿相关(各<0.001)。至少在每 2320 人中发现一种预测致病性变异。p.(Gly624Asp)在欧洲人中占变异的近一半(16/33,48%)。大多数变异(59/59,92%)具有潜在减轻临床影响的生化特征。预测致病性杂合变体影响人群的 1/106,与正常供体肾活检标本中发现的薄基底膜肾病一致。预测致病性复合杂合变体发生在每 88866 人中 1 例,双基因变体至少发生在每 44793 例中 1 例。
预测致病性变异的频率提示了 Alport 综合征的人群频率,但必须考虑个体变异的疾病外显率以及已诊断疾病和非甘氨酸取代的可能性进行调整。疾病外显率可能取决于其他遗传和环境因素。