Division of Pediatric Rheumatology/Immunology, Washington University of School of Medicine, St Louis, MO, USA.
Present Address: Department of Pediatric and Adolescent Medicine, Division of Pediatric Rheumatology, Mayo Clinic, Rochester, MN, USA.
Pediatr Rheumatol Online J. 2021 Aug 17;19(1):127. doi: 10.1186/s12969-021-00615-0.
High-intensity glucocorticoid regimens are commonly used to induce and maintain remission in Juvenile Dermatomyositis but are associated with several adverse side-effects. Evidence-based treatment guidelines from North American and European pediatric rheumatology research societies both advocate induction with intravenous pulse steroids followed by high dose oral steroids (2 mg/kg/day), which are then tapered. This study reports the time to disease control with reduced glucocorticoid dosing.
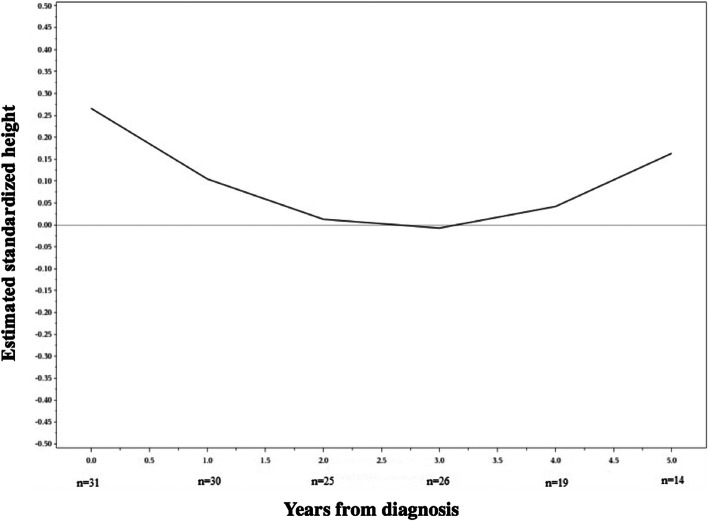
We retrospectively reviewed the records at a single tertiary-care children's hospital of patients diagnosed with Juvenile Dermatomyositis between 2000 and 2014 who had a minimum of 2 years of follow-up. The primary outcome measure was time to control of muscle and skin disease. Additional outcome measures included glucocorticoid dosing, effect of treatment on height, frequency of calcinosis, and complications from treatment.
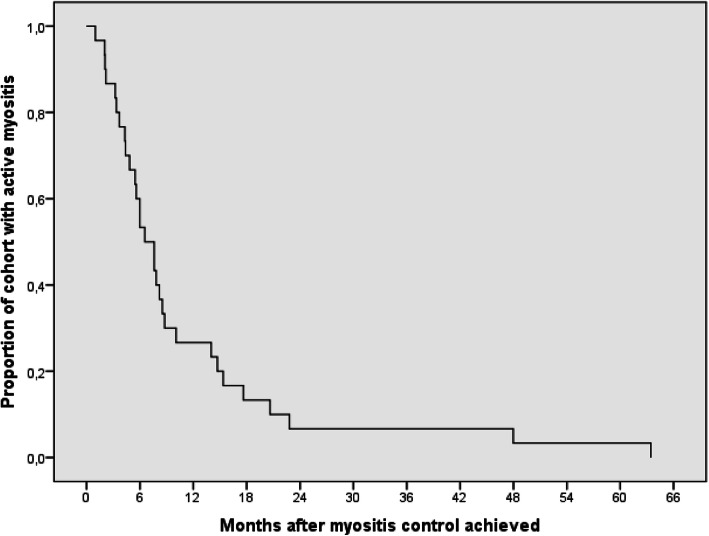
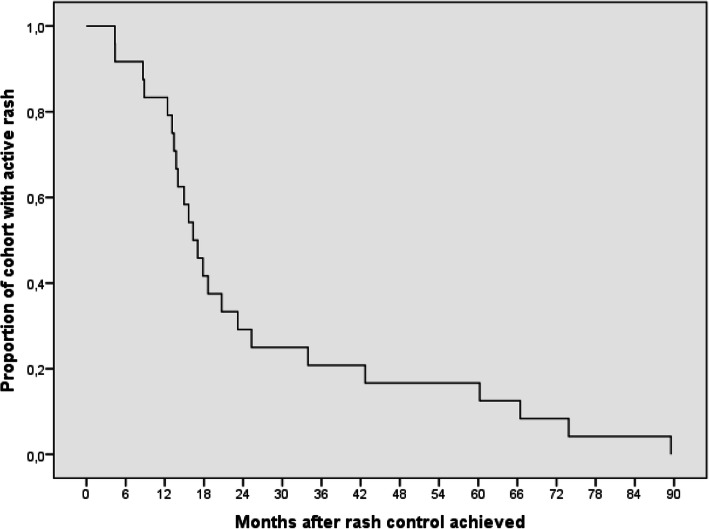
Of the 69 patients followed during the study period, 31 fulfilled inclusion criteria. Median length of follow-up was 4.58 years, (IQR 3-7.5). Myositis control was achieved in a median of 7.1 months (IQR 0.9-63.4). Cutaneous disease control was achieved in a median of 16.7 months (IQR 4.3-89.5). The median starting dose of glucocorticoids was 0.85 mg/kg/day, (IQR 0.5-1.74). The median duration of steroid treatment was 9.1 months, (IQR 4.7-17.4), while the median duration of any pharmacotherapy was 29.2 months (IQR 10.4 to 121.3). Sustained disease control off medications was achieved in 21/31 (68%) patients by the end of review. Persistent calcinosis was identified in only one patient (3%).
Current accepted treatment paradigms for Juvenile Dermatomyositis include oral glucocorticoids beginning at 2 mg/kg/day and reduced over a prolonged time period. However, our results suggest that treatment using reduced doses and duration with early use of steroid-sparing agents is comparably effective in achieving favorable outcomes in Juvenile Dermatomyositis.
高强度糖皮质激素方案常用于诱导和维持幼年皮肌炎的缓解,但与多种不良反应有关。北美和欧洲儿科风湿病研究协会的循证治疗指南均主张采用静脉脉冲类固醇诱导,然后使用高剂量口服类固醇(2mg/kg/天),随后逐渐减少剂量。本研究报告了减少糖皮质激素剂量时疾病控制的时间。
我们回顾性分析了 2000 年至 2014 年期间在一家三级儿童医院诊断为幼年皮肌炎且至少随访 2 年的患者的病历。主要结局指标是肌肉和皮肤疾病控制的时间。其他结局指标包括糖皮质激素剂量、治疗对身高的影响、钙沉积的频率以及治疗相关并发症。
在研究期间,69 例患者中有 31 例符合纳入标准。中位随访时间为 4.58 年(IQR 3-7.5)。中位肌炎控制时间为 7.1 个月(IQR 0.9-63.4)。皮肤疾病控制的中位时间为 16.7 个月(IQR 4.3-89.5)。糖皮质激素起始剂量的中位数为 0.85mg/kg/天(IQR 0.5-1.74)。类固醇治疗的中位时间为 9.1 个月(IQR 4.7-17.4),而任何药物治疗的中位时间为 29.2 个月(IQR 10.4-121.3)。在审查结束时,21/31(68%)名患者停药后持续疾病控制。只有 1 名患者(3%)持续存在钙沉积。
目前幼年皮肌炎的治疗方案包括口服糖皮质激素,起始剂量为 2mg/kg/天,然后在较长时间内逐渐减少剂量。然而,我们的结果表明,使用低剂量和短疗程,并早期使用类固醇节约剂的治疗方案,在幼年皮肌炎中同样能取得良好的效果。