Department of Reproduction Regulation, Beijing Obstetrics and Gynecology Hospital, Capital Medical University, Beijing, 100026, China.
Department of Radiology, Beijing Obstetrics and Gynecology Hospital, Capital Medical University, Beijing, 100026, China.
BMC Pregnancy Childbirth. 2021 Aug 18;21(1):568. doi: 10.1186/s12884-021-04017-8.
Pregnancy termination during the second trimester in patients with placenta previa and placenta accreta spectrum (PAS) is a complex and challenging clinical problem. Based on our literature review, there has been a relative increase in the number of such cases being treated by hysterotomy and/or local uterine lesion resection and repair. In the present study, a retrospective analysis was conducted to compare the clinical outcomes when different management strategies were used to terminate pregnancy in the patients with placenta previa and PAS.
A total of 51 patients who underwent pregnancy termination in the second trimester in Beijing Obstetrics and Gynecology Hospital between June 2013 and December 2018 were retrospectively analyzed in this study. All patients having previous caesarean delivery (CD) were diagnosed with placenta previa status and PAS.
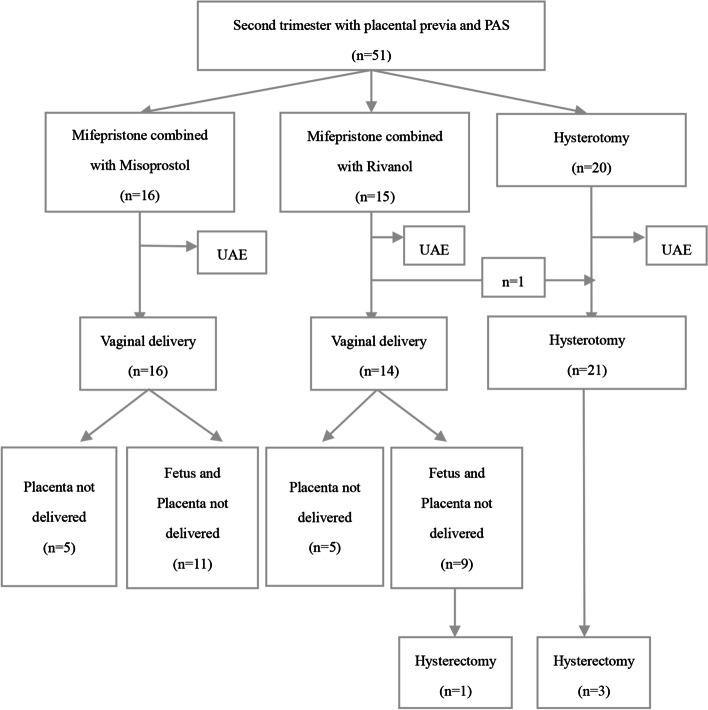
① Among the 51 patients, 16 cases received mifepristone and misoprostol medical termination, 15 cases received mifepristone and Rivanol medical termination, but 1 of them was transferred to hysterotomy due to failed labor induction, another 20 cases were performed planned hysterotomy. There was no placenta percreta cases and uterine artery embolization (UAE) was all performed before surgery.② There were 31 cases who underwent medical termination and 30 cases were vaginal delivery. Dilation and evacuation (D&E) were used in 20 cases of medical abortion failure and in all 30 cases of difficult manual removal of placental tissue. ③ A statistically significant difference was found among the three different strategies in terms of gestational weeks, the type of placenta previa status, main operative success rate and β-HCG regression time (P < 0.05). ④ There were 4(7.8%) cases who were taken up for hysterectomy because of life-threatening bleeding or severe bacteremia during or after delivery and hysterotomy. The uterus was preserved with the implanted placenta partly or completely left in situ in 47(92.2%) cases. Combined medical and/or surgical management were used for the residual placenta and the time of menstrual recovery was 52(range: 33 to 86) days after pregnancy termination.
Terminating a pregnancy by vaginal delivery through medical induction of labor may be feasible if clinicians have an overall understanding of gestational age, the type of placenta previa status, the type of placenta accreta, and patients concerns about preserving fertility. A collaborative team effort in tertiary medical centers with a very experience MDT and combined application of multiple methods is required to optimize patient outcomes.
胎盘前置和胎盘植入谱系(PAS)患者在妊娠中期行终止妊娠是一个复杂且具有挑战性的临床问题。基于我们的文献回顾,采用剖宫产术和/或局部子宫病灶切除和修复治疗的此类病例数量相对增加。本研究对不同管理策略用于治疗胎盘前置和 PAS 患者中期妊娠终止的临床结局进行了回顾性分析。
本研究回顾性分析了 2013 年 6 月至 2018 年 12 月期间在北京妇产医院接受中期妊娠终止的 51 例患者。所有有既往剖宫产史的患者均诊断为胎盘前置状态和 PAS。
①51 例患者中,16 例采用米非司酮和米索前列醇药物终止妊娠,15 例采用米非司酮和利凡诺药物终止妊娠,但 1 例因引产失败转为剖宫产,20 例计划行剖宫产。无胎盘植入病例,所有患者均在术前进行了子宫动脉栓塞术(UAE)。②31 例接受药物终止妊娠,30 例经阴道分娩。药物流产失败 20 例采用扩宫刮宫术(D&E),30 例胎盘组织徒手难以取出均采用 D&E。③三种不同策略在孕周、胎盘前置类型、主要手术成功率和β-HCG 回归时间方面差异有统计学意义(P<0.05)。④分娩或剖宫产术中或术后因危及生命的出血或严重菌血症而接受子宫切除术的患者有 4 例(7.8%)。47 例(92.2%)患者保留了子宫,部分或完全原位保留了植入胎盘。对残留胎盘采用联合药物和/或手术治疗,终止妊娠后月经恢复时间为 52 天(范围:33 至 86 天)。
如果临床医生全面了解孕周、胎盘前置类型、胎盘植入类型以及患者对保留生育能力的关注,通过药物诱导分娩行经阴道分娩终止妊娠可能是可行的。三级医疗中心的协作团队需要具备丰富的多学科诊疗经验,综合应用多种方法,以优化患者结局。