Faculty of Medicine, Hebrew University of Jerusalem, Jerusalem, Israel.
Diabetes Unit, Department of Endocrinology and Metabolism, Hadassah Medical Center, Jerusalem, Israel.
Cardiovasc Diabetol. 2021 Aug 18;20(1):169. doi: 10.1186/s12933-021-01362-y.
Randomized controlled trials showed that sodium/glucose cotransporter-2 inhibitors (SGLT2i) protect the heart and kidney in an array of populations with type 2 diabetes (T2D) and increased cardiorenal risk. However, the extent of these benefits also in lower kidney-risk T2D populations needs further investigation.
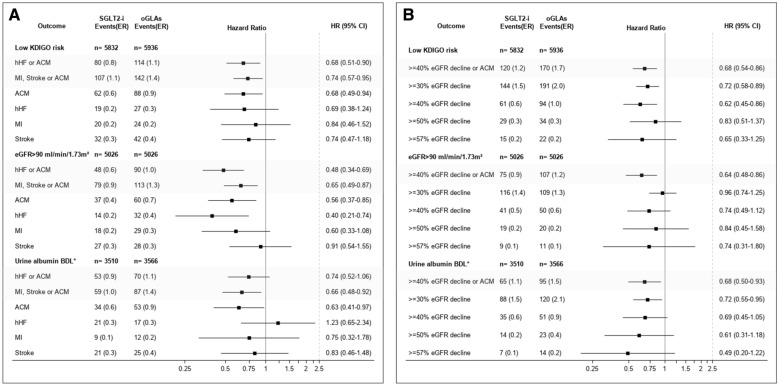
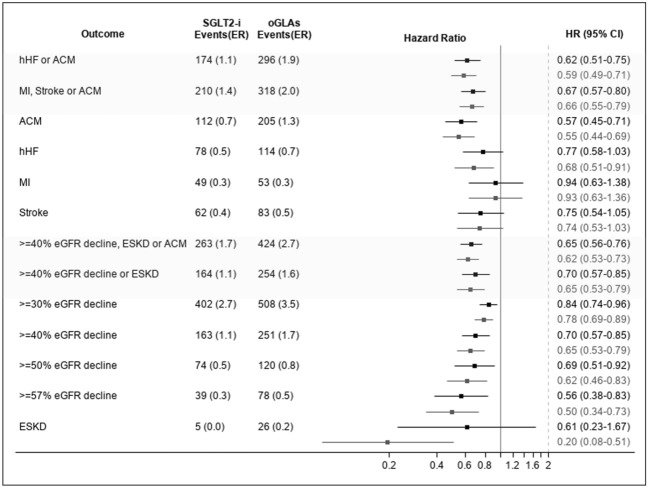
Members of Maccabi Healthcare Systems listed in their T2D registry who initiated new glucose lowering agents (GLA), were divided into SGLT2i initiators and other GLAs (oGLAs). Groups were propensity score-matched by baseline demographic and medical characteristics. Two composite cardiovascular outcomes were defined: all-cause mortality (ACM) or hospitalization for heart failure (hHF); and ACM, myocardial infraction (MI) or stroke. The cardiorenal outcome was: ACM, new end-stage kidney disease (ESKD) or ≥ 40% reduction from baseline estimated glomerular filtration rate (eGFR). Renal-specific outcome was new ESKD or ≥ 40% eGFR reduction. Single components of cardiovascular and kidney outcomes were also assessed. Three subgroup definitions of low baseline kidney-risk were used: eGFR > 90 ml/min/1.73 m; urinary albumin below detectable levels; and low risk according to Kidney Disease: Improving Global Outcomes (KDIGO) classification. Analyses were performed utilizing an unadjusted model, and a model adjusted to baseline eGFR and urinary albumin-to-creatinine ratio.
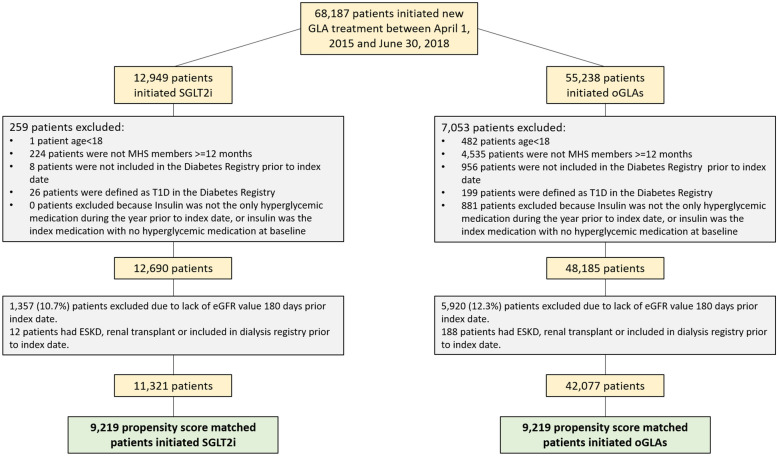
Between April 1, 2015 and June 30, 2018; 68,187 patients initiated new GLAs - 11,321 SGLT2i initiators and 42,077 oGLAs initiators were eligible. Propensity score-matching yielded two comparable cohorts; each included 9219 participants. Median follow-up was 1.7 years. Compared to oGLAs, SGLT2i initiators had lower incidence of ACM or hHF [HR = 0.62]; ACM, MI or stroke [0.67]; the cardiorenal outcome [0.65]; and the renal-specific outcome [0.70]. SGLT2i initiators also had lower risk for ACM, hHF and ≥ 30%, ≥ 40%, ≥ 50%, ≥ 57% eGFR reduction. No difference between groups was observed for MI or stroke. In the low baseline kidney-risk subgroups, SGLT2i initiation was generally associated with lower risk of the cardiovascular and cardiorenal outcomes, driven mainly by lower ACM incidence.
Our findings in the general population of patients with T2D demonstrates lower risk of cardiorenal outcomes associated with initiation of SGLT2i compared with oGLAs, including specifically in patients with low baseline kidney-risk.
随机对照试验表明,钠/葡萄糖共转运蛋白-2 抑制剂(SGLT2i)在多种 2 型糖尿病(T2D)和心血管肾风险增加的人群中可保护心脏和肾脏。然而,这些益处的程度在低肾脏风险的 T2D 人群中还需要进一步研究。
在 Maccabi 医疗保健系统登记的开始使用新型降血糖药物(GLA)的 2 型糖尿病患者中,将其分为 SGLT2i 使用者和其他 GLA(oGLAs)使用者。两组患者根据基线人口统计学和医疗特征进行倾向评分匹配。定义了两个复合心血管结局:全因死亡率(ACM)或心力衰竭住院(hHF);以及 ACM、心肌梗死(MI)或中风。心血管肾结局为:ACM、新发终末期肾病(ESKD)或肾小球滤过率(eGFR)基线值下降≥40%。肾脏特异性结局为新发 ESKD 或 eGFR 下降≥40%。还评估了心血管和肾脏结局的单一组成部分。使用三种低基线肾脏风险的定义:eGFR>90ml/min/1.73m;尿白蛋白低于可检测水平;以及根据肾脏病:改善全球结果(KDIGO)分类的低风险。利用未调整模型和调整至基线 eGFR 和尿白蛋白/肌酐比值的模型进行分析。
2015 年 4 月 1 日至 2018 年 6 月 30 日期间,有 68187 名患者开始使用新型 GLA-其中 11321 名为 SGLT2i 使用者,42077 名为 oGLAs 使用者符合条件。倾向评分匹配产生了两个可比队列;每个队列都包括 9219 名参与者。中位随访时间为 1.7 年。与 oGLAs 相比,SGLT2i 使用者的 ACM 或 hHF 发生率较低[HR=0.62];ACM、MI 或中风[0.67];心血管肾结局[0.65];肾脏特异性结局[0.70]。SGLT2i 使用者的 ACM、hHF 和 eGFR 降低≥30%、≥40%、≥50%、≥57%的风险也较低。两组间 MI 或中风的风险无差异。在低基线肾脏风险亚组中,SGLT2i 的使用通常与心血管和心血管肾结局的风险降低相关,主要归因于 ACM 发生率的降低。
在 2 型糖尿病患者的一般人群中,与 oGLAs 相比,SGLT2i 的使用与较低的心血管肾结局风险相关,包括在基线肾脏风险较低的患者中。