University of Toronto, Toronto, ON, Canada.
University of Nantes, Nantes, France.
Diabetologia. 2021 Jun;64(6):1256-1267. doi: 10.1007/s00125-021-05407-5. Epub 2021 Mar 4.
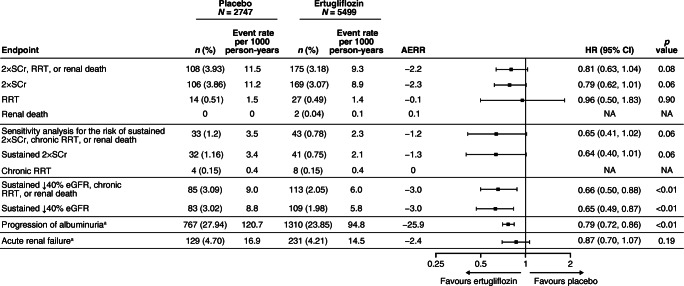
AIMS/HYPOTHESIS: In previous work, we reported the HR for the risk (95% CI) of the secondary kidney composite endpoint (time to first event of doubling of serum creatinine from baseline, renal dialysis/transplant or renal death) with ertugliflozin compared with placebo as 0.81 (0.63, 1.04). The effect of ertugliflozin on exploratory kidney-related outcomes was evaluated using data from the eValuation of ERTugliflozin effIcacy and Safety CardioVascular outcomes (VERTIS CV) trial (NCT01986881).
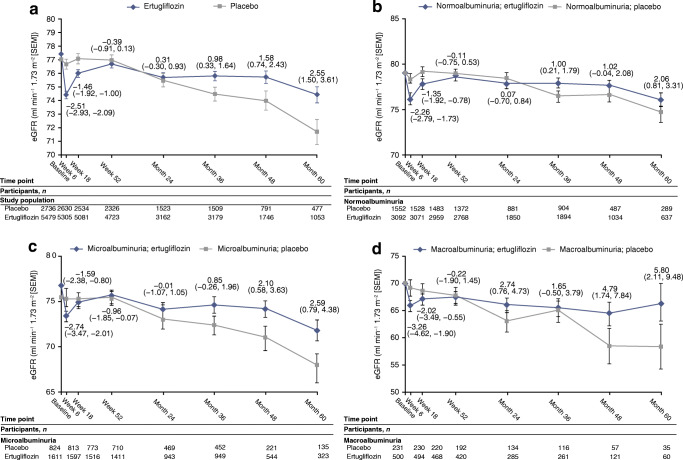
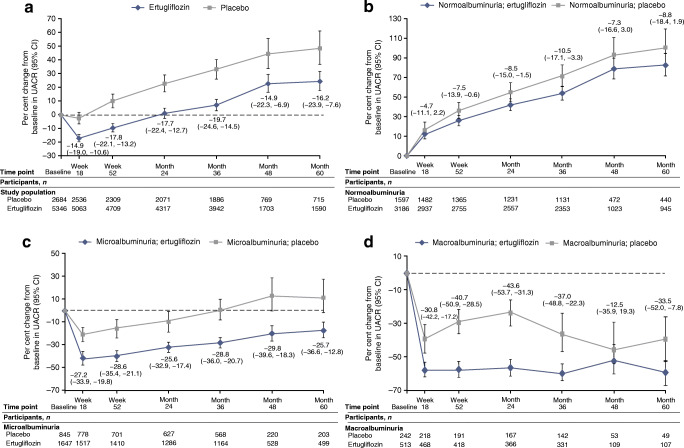
Individuals with type 2 diabetes mellitus and established atherosclerotic CVD were randomised to receive ertugliflozin 5 mg or 15 mg (observations from both doses were pooled), or matching placebo, added on to existing treatment. The kidney composite outcome in VERTIS CV (reported previously) was time to first event of doubling of serum creatinine from baseline, renal dialysis/transplant or renal death. The pre-specified exploratory composite outcome replaced doubling of serum creatinine with sustained 40% decrease from baseline in eGFR. In addition, the impact of ertugliflozin on urinary albumin/creatinine ratio (UACR) and eGFR over time was assessed.
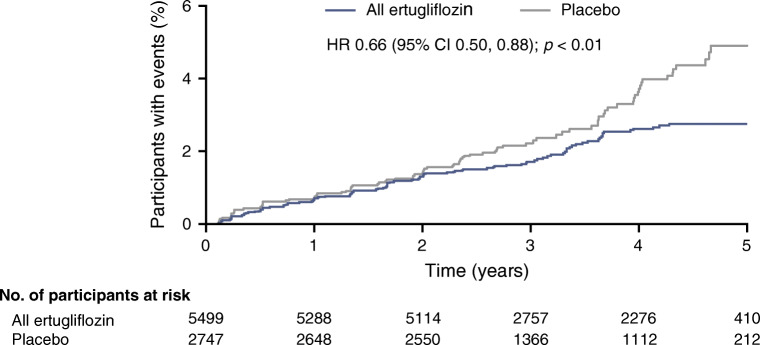
A total of 8246 individuals were randomised and followed for a mean of 3.5 years. The exploratory kidney composite outcome of sustained 40% reduction from baseline in eGFR, chronic kidney dialysis/transplant or renal death occurred at a lower event rate (events per 1000 person-years) in the ertugliflozin group than with the placebo group (6.0 vs 9.0); the HR (95% CI) was 0.66 (0.50, 0.88). At 60 months, in the ertugliflozin group, placebo-corrected changes from baseline (95% CIs) in UACR and eGFR were -16.2% (-23.9, -7.6) and 2.6 ml min [1.73 m] (1.5, 3.6), respectively. Ertugliflozin was associated with a consistent decrease in UACR and attenuation of eGFR decline across subgroups, with a suggested larger effect observed in the macroalbuminuria and Kidney Disease: Improving Global Outcomes in Chronic Kidney Disease (KDIGO CKD) high/very high-risk subgroups.
CONCLUSIONS/INTERPRETATION: Among individuals with type 2 diabetes and atherosclerotic CVD, ertugliflozin reduced the risk for the pre-specified exploratory composite renal endpoint and was associated with preservation of eGFR and reduced UACR.
ClinicalTrials.gov NCT01986881.
目的/假设:在之前的研究中,我们报告了与安慰剂相比,依格列净的风险(95%CI)的次要肾脏复合终点(血清肌酐从基线翻倍的首次事件、肾脏透析/移植或肾脏死亡)的风险比为 0.81(0.63,1.04)。使用来自 eValuation of ERTugliflozin effIcacy and Safety CardioVascular outcomes(VERTIS CV)试验(NCT01986881)的数据,评估了依格列净对探索性肾脏相关结局的影响。
2 型糖尿病和已确诊的动脉粥样硬化性心血管疾病患者被随机分配接受依格列净 5mg 或 15mg(两种剂量的观察结果均被汇总)或匹配的安慰剂,加用现有治疗。VERTIS CV 中的肾脏复合终点(先前报告过)是血清肌酐从基线翻倍、肾脏透析/移植或肾脏死亡的首次事件。预先指定的探索性复合终点用 eGFR 从基线持续下降 40%代替血清肌酐翻倍。此外,还评估了依格列净对尿白蛋白/肌酐比值(UACR)和 eGFR 随时间的影响。
共有 8246 名患者被随机分配并平均随访 3.5 年。与安慰剂组相比,依格列净组从基线持续下降 40%的 eGFR、慢性肾脏透析/移植或肾脏死亡的探索性肾脏复合终点的事件发生率较低(每 1000 人年的事件数)(6.0 比 9.0);风险比(95%CI)为 0.66(0.50,0.88)。在 60 个月时,依格列净组 UACR 和 eGFR 从基线的校正变化(95%CI)分别为-16.2%(-23.9,-7.6)和 2.6ml·min[-1.73·m](1.5,3.6)。依格列净与 UACR 持续下降和 eGFR 下降幅度降低有关,在大量白蛋白尿和肾脏病:改善全球肾脏病预后组织(KDIGO CKD)高/极高风险亚组中观察到更大的效果。
结论/解释:在 2 型糖尿病和动脉粥样硬化性心血管疾病患者中,依格列净降低了预先指定的探索性复合肾脏终点的风险,并与 eGFR 的保留和 UACR 的降低有关。
ClinicalTrials.gov NCT01986881。