Wassink Guido, Davidson Joanne O, Crisostomo Alyssa, Zhou Kelly Q, Galinsky Robert, Dhillon Simerdeep K, Lear Christopher A, Bennet Laura, Gunn Alistair J
Department of Physiology, The University of Auckland, Auckland, New Zealand.
The Ritchie Centre, Hudson Institute of Medical Research, Victoria, Australia.
Brain Commun. 2021 Jul 29;3(3):fcab172. doi: 10.1093/braincomms/fcab172. eCollection 2021.
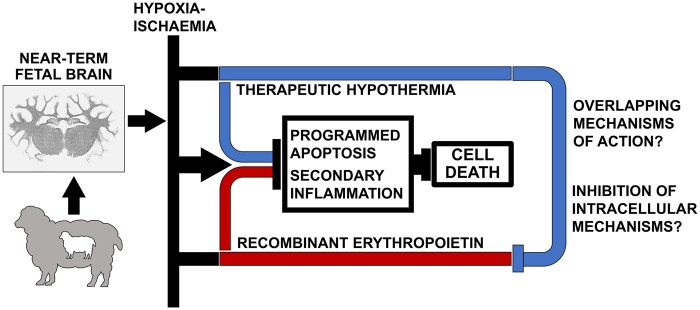
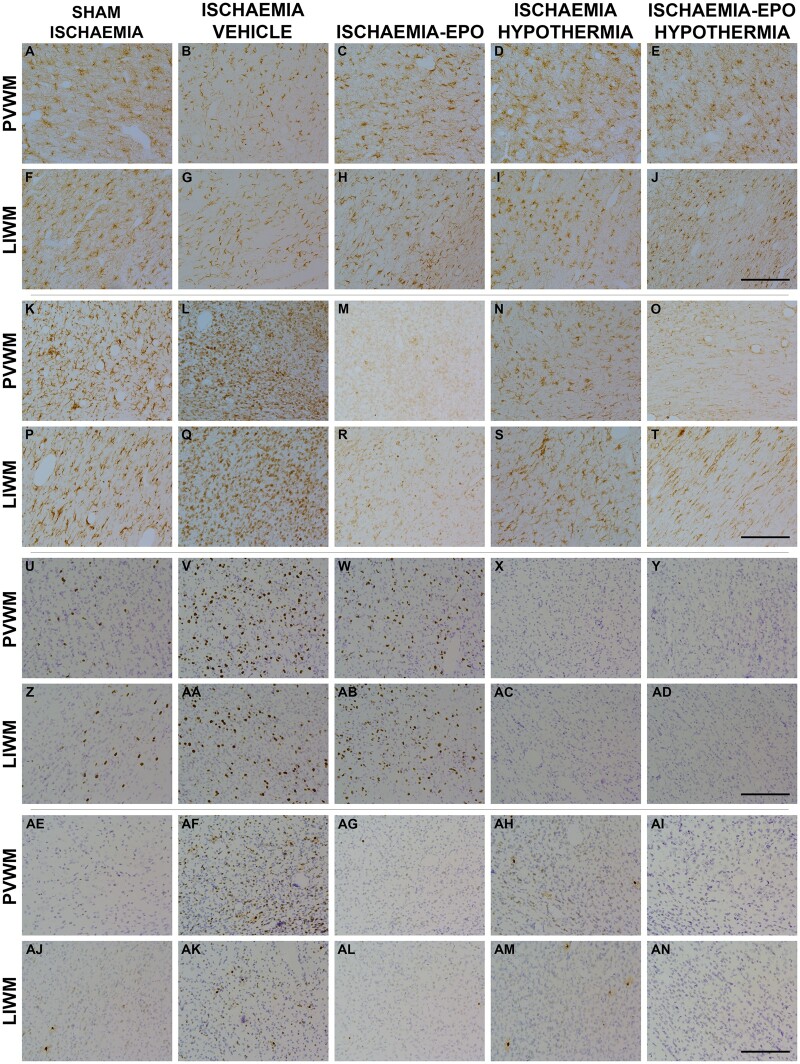
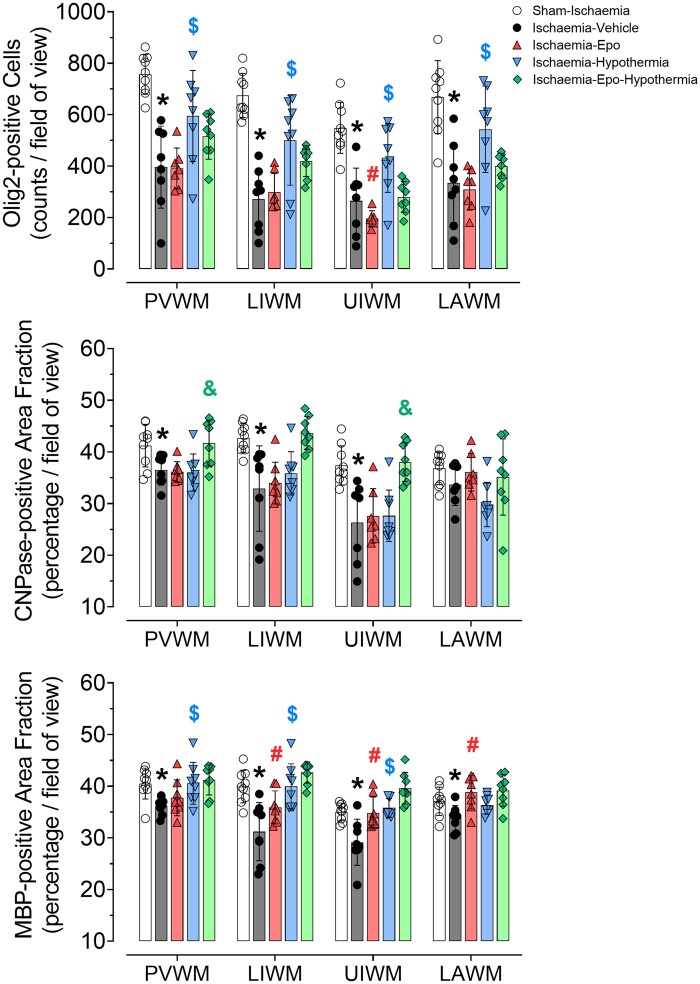
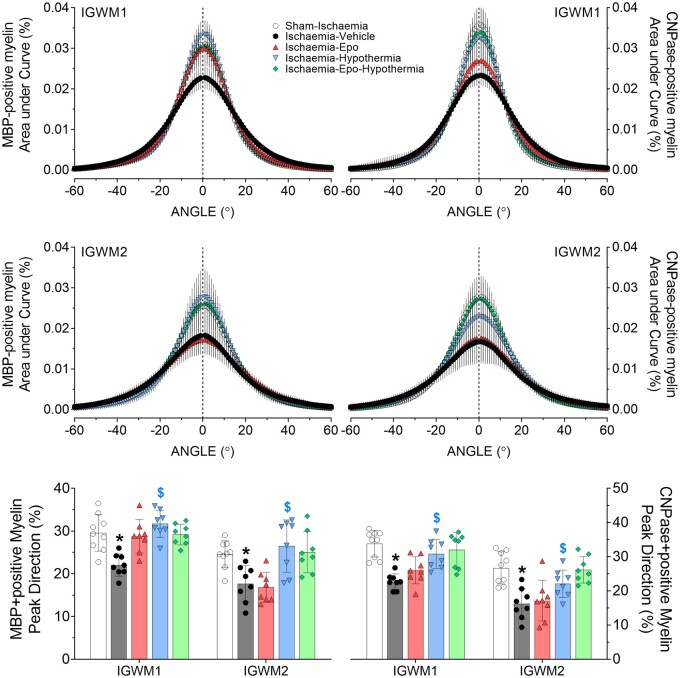
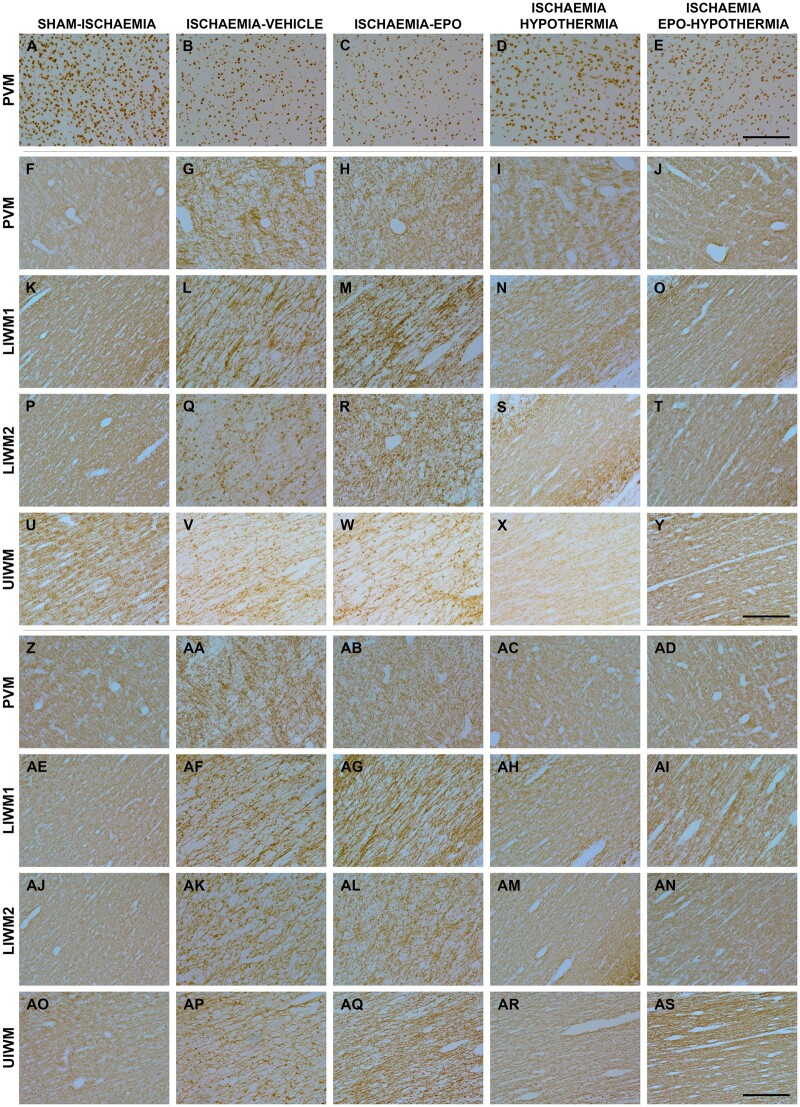
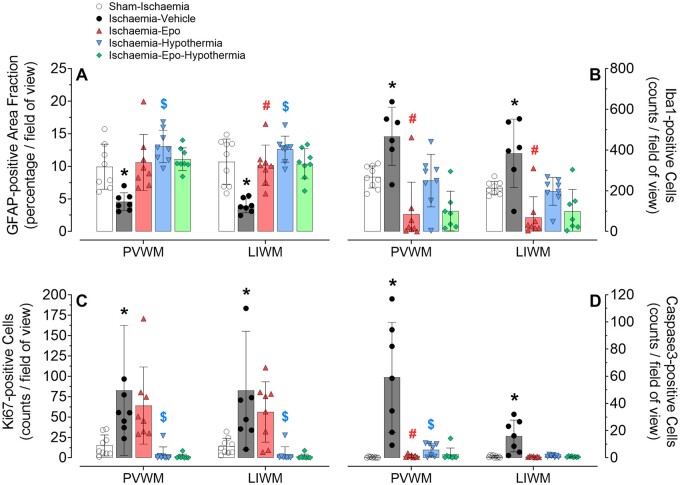
Therapeutic hypothermia for hypoxic-ischaemic encephalopathy provides partial white matter protection. Recombinant erythropoietin reduces demyelination after hypoxia-ischaemia, but it is unclear whether adjunct erythropoietin treatment can further improve outcomes after therapeutic hypothermia. Term-equivalent fetal sheep received sham-ischaemia ( = 9) or cerebral ischaemia for 30 min (ischaemia-vehicle, = 8), followed by intravenous infusion of recombinant erythropoietin (ischaemia-Epo, = 8; 5000 IU/kg bolus dose, then 833.3 IU/kg/h), cerebral hypothermia (ischaemia-hypothermia, = 8), or recombinant erythropoietin plus hypothermia (ischaemia-Epo-hypothermia, = 8), from 3 to 72 h post-ischaemia. Foetal brains were harvested at 7 days after cerebral ischaemia. Ischaemia was associated with marked loss of total Olig2-positive oligodendrocytes with reduced density of myelin and linearity of the white matter tracts ( < 0.01), and microglial induction and increased caspase-3-positive apoptosis. Cerebral hypothermia improved the total number of oligodendrocytes and restored myelin basic protein ( < 0.01), whereas recombinant erythropoietin partially improved myelin basic protein density and tract linearity. Both interventions suppressed microgliosis and caspase-3 ( < 0.05). Co-treatment improved 2',3'-cyclic-nucleotide 3'-phosphodiesterase-myelin density compared to hypothermia, but had no other additive effect. These findings suggest that although hypothermia and recombinant erythropoietin independently protect white matter after severe hypoxia-ischaemia, they have partially overlapping anti-inflammatory and anti-apoptotic effects, with little additive benefit of combination therapy.
治疗性低温对缺氧缺血性脑病具有部分白质保护作用。重组促红细胞生成素可减少缺氧缺血后的脱髓鞘,但尚不清楚联合促红细胞生成素治疗能否在治疗性低温后进一步改善预后。足月胎羊接受假缺血(n = 9)或30分钟的脑缺血(缺血-载体组,n = 8),随后在缺血后3至72小时静脉输注重组促红细胞生成素(缺血-Epo组,n = 8;5000 IU/kg推注剂量,然后833.3 IU/kg/h)、脑低温(缺血-低温组,n = 8)或重组促红细胞生成素加低温(缺血-Epo-低温组,n = 8)。在脑缺血7天后收获胎脑。缺血与总Olig2阳性少突胶质细胞显著减少、髓鞘密度降低和白质束线性降低相关(P < 0.01),以及小胶质细胞诱导和caspase-3阳性凋亡增加。脑低温改善了少突胶质细胞总数并恢复了髓鞘碱性蛋白(P < 0.01),而重组促红细胞生成素部分改善了髓鞘碱性蛋白密度和束线性。两种干预均抑制了小胶质细胞增生和caspase-3(P < 0.05)。与低温相比,联合治疗改善了2',3'-环核苷酸3'-磷酸二酯酶-髓鞘密度,但没有其他相加效应。这些发现表明,尽管低温和重组促红细胞生成素在严重缺氧缺血后独立保护白质,但它们具有部分重叠的抗炎和抗凋亡作用,联合治疗几乎没有相加益处。