Pang Raymand, Avdic-Belltheus Adnan, Meehan Christopher, Martinello Kathryn, Mutshiya Tatenda, Yang Qin, Sokolska Magdalena, Torrealdea Francisco, Hristova Mariya, Bainbridge Alan, Golay Xavier, Juul Sandra E, Robertson Nicola J
Department of Neonatology, Institute for Women's Health, University College London, London, UK.
Department of Medical Physics and Biomedical Engineering, University College London Hospitals, London, UK.
Brain Commun. 2020 Dec 1;3(1):fcaa211. doi: 10.1093/braincomms/fcaa211. eCollection 2021.
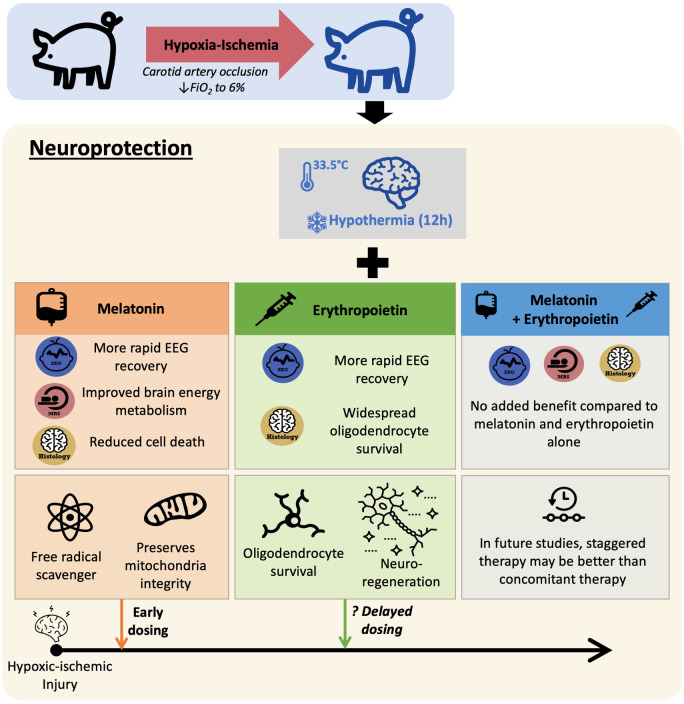
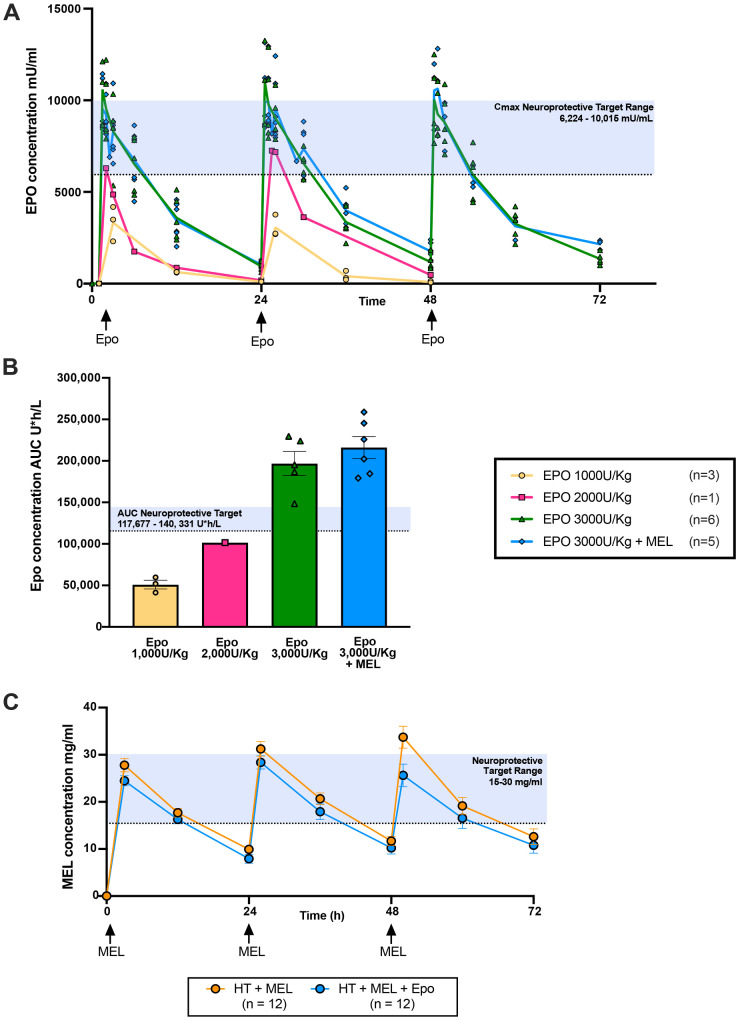
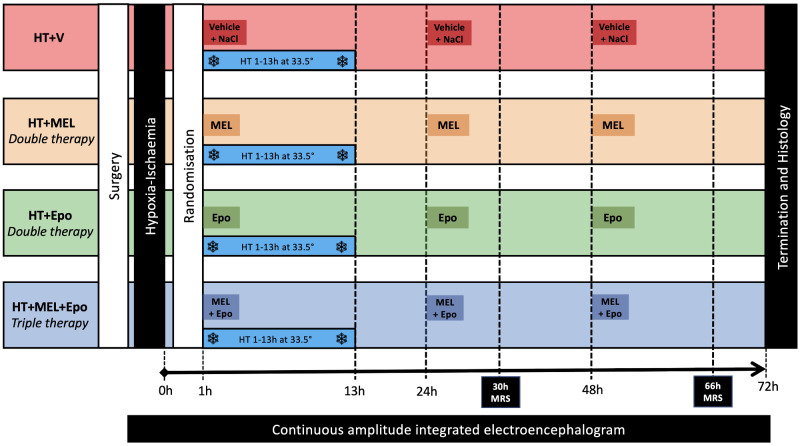
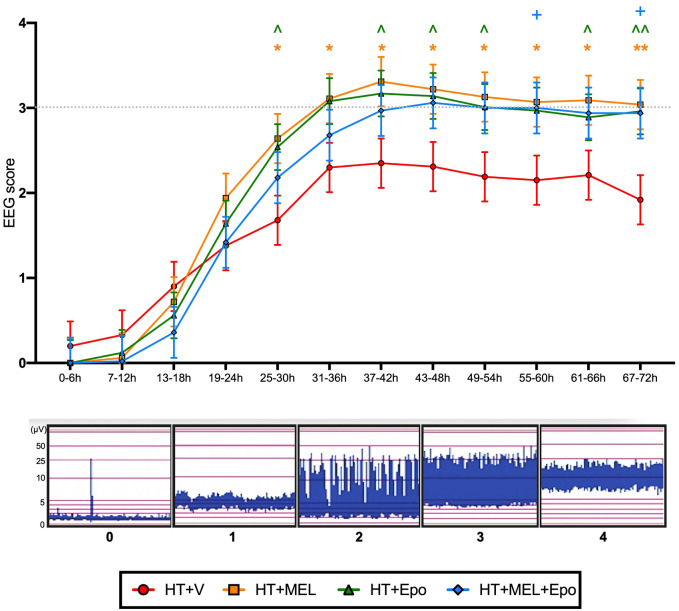
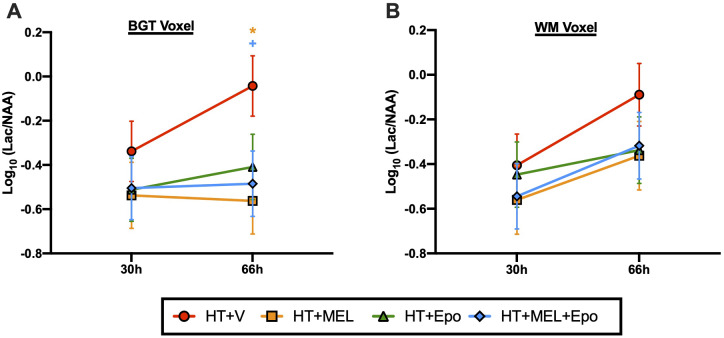
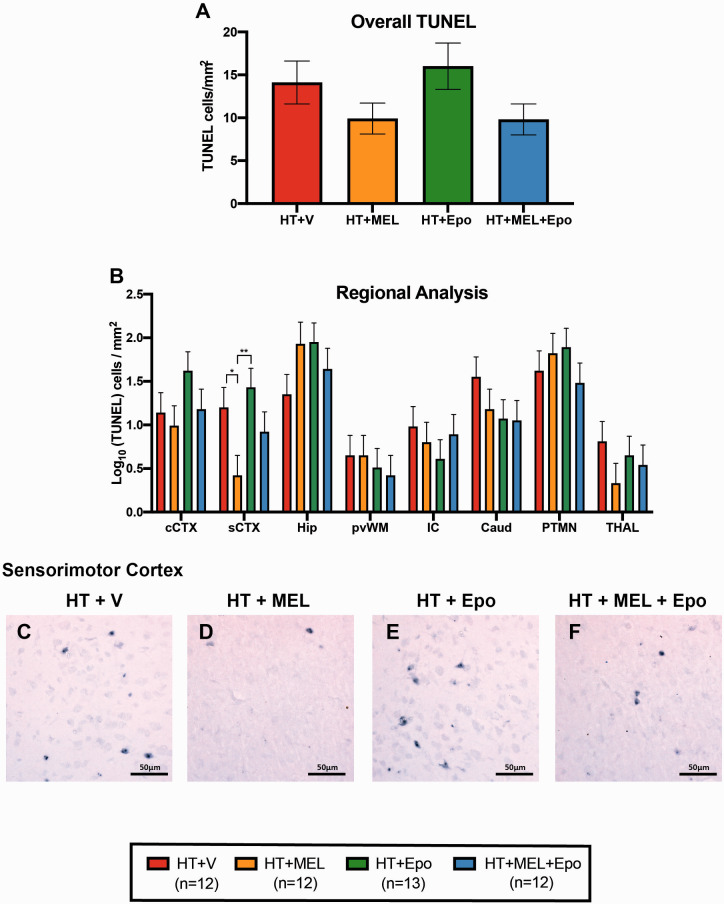
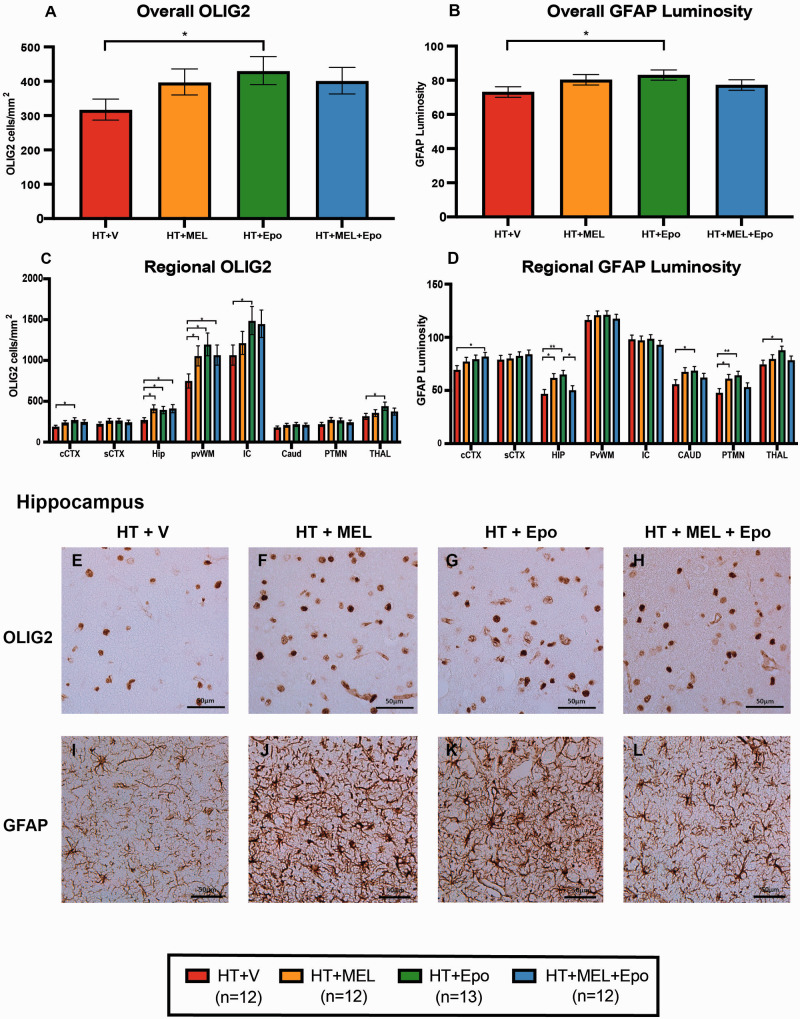
As therapeutic hypothermia is only partially protective for neonatal encephalopathy, safe and effective adjunct therapies are urgently needed. Melatonin and erythropoietin show promise as safe and effective neuroprotective therapies. We hypothesized that melatonin and erythropoietin individually augment 12-h hypothermia ( therapies) and hypothermia + melatonin + erythropoietin () leads to optimal brain protection. Following carotid artery occlusion and hypoxia, 49 male piglets (<48 h old) were randomized to: (i) hypothermia + vehicle ( = 12), (ii) hypothermia + melatonin (20 mg/kg over 2 h) ( = 12), (iii) hypothermia + erythropoietin (3000 U/kg bolus) ( = 13) or (iv) ( = 12). Melatonin, erythropoietin or vehicle were given at 1, 24 and 48 h after hypoxia-ischaemia. Hypoxia-ischaemia severity was similar across groups. Therapeutic levels were achieved 3 hours after hypoxia-ischaemia for melatonin (15-30 mg/l) and within 30 min of erythropoietin administration (maximum concentration 10 000 mU/ml). Compared to hypothermia + vehicle, we observed faster amplitude-integrated EEG recovery from 25 to 30 h with hypothermia + melatonin ( = 0.02) and hypothermia + erythropoietin ( = 0.033) and from 55 to 60 h with ( = 0.042). Magnetic resonance spectroscopy lactate/-acetyl aspartate peak ratio was lower at 66 h in hypothermia + melatonin ( = 0.012) and ( = 0.032). With hypothermia + melatonin, terminal deoxynucleotidyl transferase-mediated deoxyuridine triphosphate nick-end labelled-positive cells were reduced in sensorimotor cortex ( = 0.017) and oligodendrocyte transcription factor 2 labelled-positive counts increased in hippocampus ( = 0.014) and periventricular white matter ( = 0.039). There was no reduction in terminal deoxynucleotidyl transferase-mediated deoxyuridine triphosphate nick-end labelled-positive cells with hypothermia + erythropoietin, but increased oligodendrocyte transcription factor 2 labelled-positive cells in 5 of 8 brain regions ( < 0.05). Overall, melatonin and erythropoietin were safe and effective adjunct therapies to hypothermia. Hypothermia + melatonin led to faster amplitude-integrated EEG recovery, amelioration of lactate/N-acetyl aspartate rise and reduction in terminal deoxynucleotidyl transferase-mediated deoxyuridine triphosphate nick-end labelled-positive cells in the sensorimotor cortex. Hypothermia + erythropoietin was in association with EEG recovery and was most effective in promoting oligodendrocyte survival. provided no added benefit over the therapies in this 72-h study. Melatonin and erythropoietin influenced cell death and oligodendrocyte survival differently, reflecting distinct neuroprotective mechanisms which may become more visible with longer-term studies. Staggering the administration of therapies with early melatonin and later erythropoietin (after hypothermia) may provide better protection; each therapy has complementary actions which may be time critical during the neurotoxic cascade after hypoxia-ischaemia.
由于治疗性低温对新生儿脑病仅具有部分保护作用,因此迫切需要安全有效的辅助治疗方法。褪黑素和促红细胞生成素有望成为安全有效的神经保护疗法。我们推测,褪黑素和促红细胞生成素单独使用可增强12小时低温治疗效果,而低温 + 褪黑素 + 促红细胞生成素联合治疗可实现最佳脑保护。在颈动脉闭塞和缺氧后,将49头雄性仔猪(<48小时龄)随机分为:(i)低温 + 赋形剂(n = 12),(ii)低温 + 褪黑素(2小时内给予20mg/kg)(n = 12),(iii)低温 + 促红细胞生成素(3000U/kg静脉推注)(n = 13)或(iv)联合治疗组(n = 12)。在缺氧缺血后1、24和48小时给予褪黑素、促红细胞生成素或赋形剂。各组缺氧缺血严重程度相似。缺氧缺血后3小时达到褪黑素治疗水平(15 - 30mg/l),促红细胞生成素给药后30分钟内达到治疗水平(最大浓度10000mU/ml)。与低温 + 赋形剂组相比,我们观察到低温 + 褪黑素组(P = 0.02)和低温 + 促红细胞生成素组(P = 0.033)在25至30小时时振幅整合脑电图恢复更快,联合治疗组在55至60小时时恢复更快(P = 0.042)。在66小时时,低温 + 褪黑素组(P = 0.012)和联合治疗组(P = 0.032)磁共振波谱乳酸/ N - 乙酰天门冬氨酸峰值比更低。低温 + 褪黑素组感觉运动皮层中末端脱氧核苷酸转移酶介导的脱氧尿苷三磷酸缺口末端标记阳性细胞减少(P = 0.017),海马体(P = 0.014)和脑室周围白质(P = 0.039)中少突胶质细胞转录因子2标记阳性细胞计数增加。低温 + 促红细胞生成素组末端脱氧核苷酸转移酶介导的脱氧尿苷三磷酸缺口末端标记阳性细胞没有减少,但在8个脑区中的5个脑区少突胶质细胞转录因子2标记阳性细胞增加(P < 0.05)。总体而言,褪黑素和促红细胞生成素是低温治疗安全有效的辅助疗法。低温 + 褪黑素组导致振幅整合脑电图恢复更快,改善乳酸/ N - 乙酰天门冬氨酸升高,并减少感觉运动皮层中末端脱氧核苷酸转移酶介导的脱氧尿苷三磷酸缺口末端标记阳性细胞。低温 + 促红细胞生成素联合治疗与脑电图恢复相关,并且在促进少突胶质细胞存活方面最有效。在这项72小时的研究中,联合治疗组相比其他治疗组未显示出额外益处。褪黑素和促红细胞生成素对细胞死亡和少突胶质细胞存活的影响不同,反映了不同的神经保护机制,长期研究可能会更明显地体现出来。错开治疗给药时间,早期给予褪黑素,后期(低温治疗后)给予促红细胞生成素可能会提供更好的保护;每种疗法具有互补作用,这在缺氧缺血后的神经毒性级联反应中可能对时间要求严格。