Hearing and Genes, Department of Otorhinolaryngology, Radboud University Medical Center, Nijmegen, The Netherlands.
Department of Human Genetics, Radboud University Medical Center, Internal Postal Code 855, P.O. Box 9101, 6500 HB, Nijmegen, The Netherlands.
Hum Genet. 2022 Apr;141(3-4):465-484. doi: 10.1007/s00439-021-02336-6. Epub 2021 Aug 19.
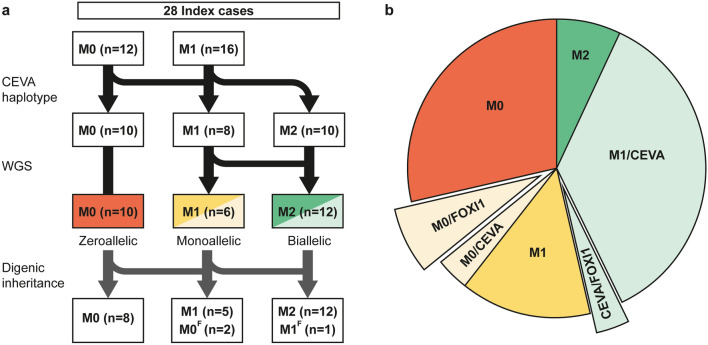
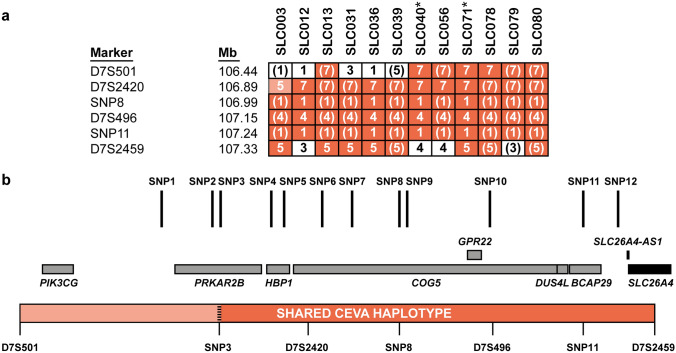
Pathogenic variants in SLC26A4 have been associated with autosomal recessive hearing loss (arHL) and a unilateral or bilateral enlarged vestibular aqueduct (EVA). SLC26A4 is the second most frequently mutated gene in arHL. Despite the strong genotype-phenotype correlation, a significant part of cases remains genetically unresolved. In this study, we investigated a cohort of 28 Dutch index cases diagnosed with HL in combination with an EVA but without (M0) or with a single (M1) pathogenic variant in SLC26A4. To explore the missing heritability, we first determined the presence of the previously described EVA-associated haplotype (Caucasian EVA (CEVA)), characterized by 12 single nucleotide variants located upstream of SLC26A4. We found this haplotype and a delimited V1-CEVA haplotype to be significantly enriched in our M1 patient cohort (10/16 cases). The CEVA haplotype was also present in two M0 cases (2/12). Short- and long-read whole genome sequencing and optical genome mapping could not prioritize any of the variants present within the CEVA haplotype as the likely pathogenic defect. Short-read whole-genome sequencing of the six M1 cases without this haplotype and the two M0/CEVA cases only revealed previously overlooked or misinterpreted splice-altering SLC26A4 variants in two cases, who are now genetically explained. No deep-intronic or structural variants were identified in any of the M1 subjects. With this study, we have provided important insights that will pave the way for elucidating the missing heritability in M0 and M1 SLC26A4 cases. For pinpointing the pathogenic effect of the CEVA haplotype, additional analyses are required addressing defect(s) at the RNA, protein, or epigenetic level.
SLC26A4 中的致病变体与常染色体隐性遗传性听力损失(arHL)和单侧或双侧扩大的前庭导水管(EVA)有关。SLC26A4 是 arHL 中第二大常突变基因。尽管基因型-表型相关性很强,但仍有很大一部分病例在遗传上无法解决。在这项研究中,我们调查了 28 名荷兰索引病例,这些病例均诊断为 HL 合并 EVA,但 SLC26A4 中不存在(M0)或存在单一(M1)致病性变体。为了探索缺失的遗传率,我们首先确定了先前描述的与 EVA 相关的单倍型(高加索 EVA(CEVA))的存在,该单倍型由位于 SLC26A4 上游的 12 个单核苷酸变体组成。我们发现该单倍型和限定的 V1-CEVA 单倍型在我们的 M1 患者队列中显著富集(16 例中有 10 例)。M0 病例中有两个(12 例中有 2 例)也存在 CEVA 单倍型。短读和长读全基因组测序和光学基因组图谱无法确定 CEVA 单倍型内存在的任何变体作为可能的致病缺陷。对没有该单倍型的六个 M1 病例和两个 M0/CEVA 病例进行短读全基因组测序,仅在两个病例中揭示了以前被忽视或误解的剪接改变的 SLC26A4 变体,现在可以从遗传学上解释这些病例。在任何 M1 受试者中均未发现深内含子或结构变体。通过这项研究,我们提供了重要的见解,为阐明 M0 和 M1 SLC26A4 病例中缺失的遗传率铺平了道路。为了确定 CEVA 单倍型的致病效应,需要进行额外的分析,以确定 RNA、蛋白质或表观遗传水平的缺陷。