Popescu Narcis I, Lupu Cristina, Lupu Florea
Arthritis and Clinical Immunology Research and.
Cardiovascular Biology Research Program, Oklahoma Medical Research Foundation, Oklahoma City, OK; and.
Blood. 2022 Mar 31;139(13):1973-1986. doi: 10.1182/blood.2020007208.
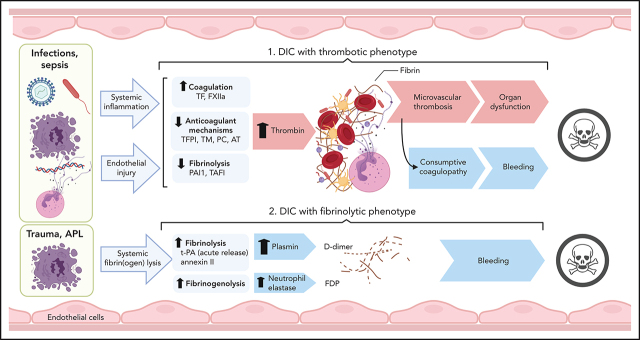
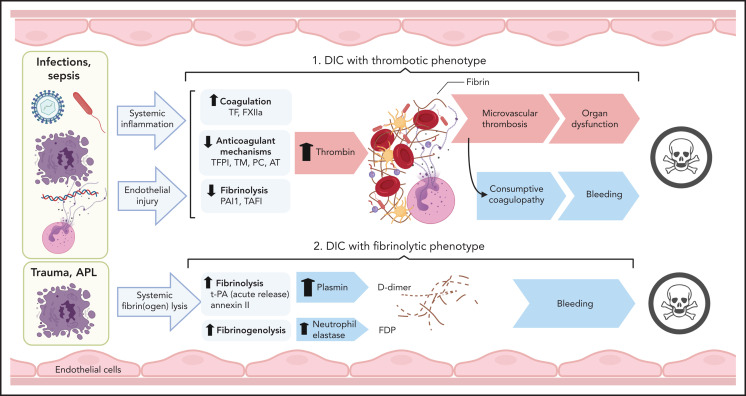
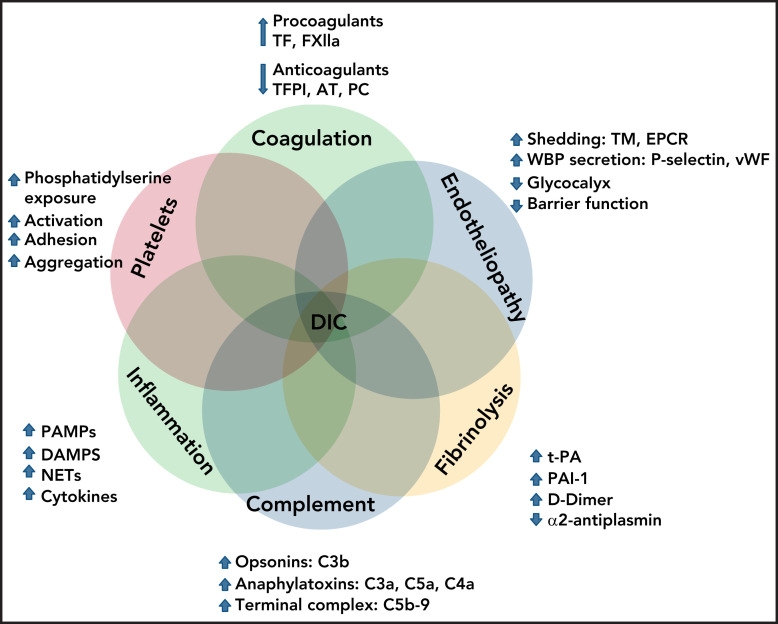
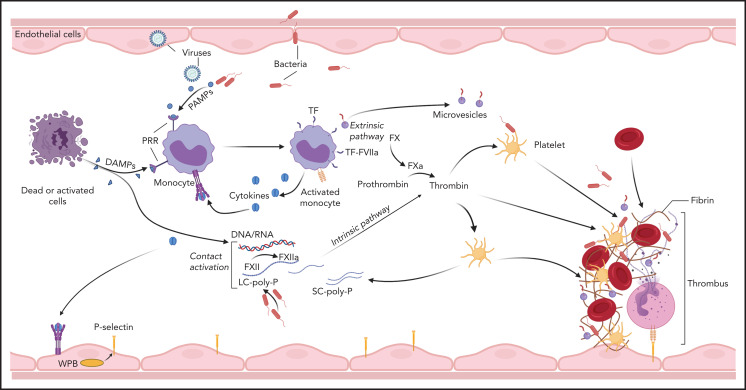
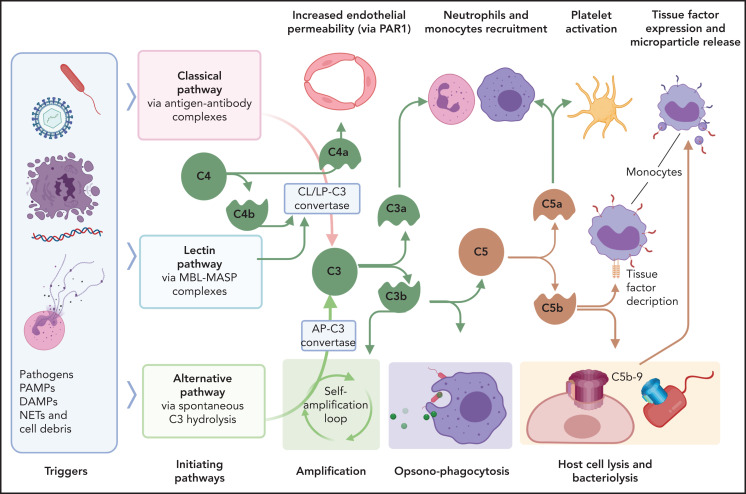
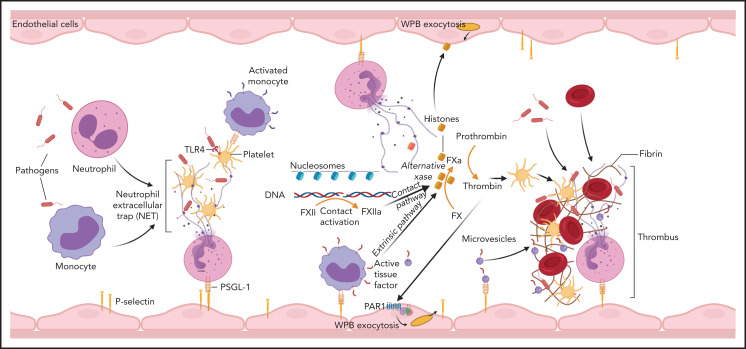
Disseminated intravascular coagulation (DIC) is a syndrome triggered by infectious and noninfectious pathologies characterized by excessive generation of thrombin within the vasculature and widespread proteolytic conversion of fibrinogen. Despite diverse clinical manifestations ranging from thrombo-occlusive damage to bleeding diathesis, DIC etiology commonly involves excessive activation of blood coagulation and overlapping dysregulation of anticoagulants and fibrinolysis. Initiation of blood coagulation follows intravascular expression of tissue factor or activation of the contact pathway in response to pathogen-associated or host-derived, damage-associated molecular patterns. The process is further amplified through inflammatory and immunothrombotic mechanisms. Consumption of anticoagulants and disruption of endothelial homeostasis lower the regulatory control and disseminate microvascular thrombosis. Clinical DIC development in patients is associated with worsening morbidities and increased mortality, regardless of the underlying pathology; therefore, timely recognition of DIC is critical for reducing the pathologic burden. Due to the diversity of triggers and pathogenic mechanisms leading to DIC, diagnosis is based on algorithms that quantify hemostatic imbalance, thrombocytopenia, and fibrinogen conversion. Because current diagnosis primarily assesses overt consumptive coagulopathies, there is a critical need for better recognition of nonovert DIC and/or pre-DIC states. Therapeutic strategies for patients with DIC involve resolution of the eliciting triggers and supportive care for the hemostatic imbalance. Despite medical care, mortality in patients with DIC remains high, and new strategies, tailored to the underlying pathologic mechanisms, are needed.
弥散性血管内凝血(DIC)是一种由感染性和非感染性病理状态引发的综合征,其特征为血管内凝血酶过度生成以及纤维蛋白原广泛的蛋白水解转化。尽管DIC有从血栓闭塞性损伤到出血倾向等多种临床表现,但其病因通常涉及凝血的过度激活以及抗凝剂和纤维蛋白溶解的重叠失调。凝血的启动是在组织因子在血管内表达或接触途径被激活后发生的,这是对病原体相关或宿主来源的损伤相关分子模式的反应。该过程通过炎症和免疫血栓形成机制进一步放大。抗凝剂的消耗和内皮稳态的破坏降低了调节控制并扩散了微血管血栓形成。无论潜在病理状态如何,患者临床DIC的发展都与病情恶化和死亡率增加相关;因此,及时识别DIC对于减轻病理负担至关重要。由于导致DIC的触发因素和致病机制多种多样,诊断基于量化止血失衡、血小板减少和纤维蛋白原转化的算法。由于目前的诊断主要评估明显的消耗性凝血病,因此迫切需要更好地识别非明显DIC和/或DIC前期状态。DIC患者的治疗策略包括消除引发触发因素以及对止血失衡进行支持性护理。尽管进行了医疗护理,DIC患者的死亡率仍然很高,需要针对潜在病理机制量身定制新的策略。