From the Department of Pediatrics, Center for Vaccine Development and Global Health, University of Maryland School of Medicine, Baltimore, Maryland.
Centre pour le Développement des Vaccins-Mali, Bamako, Mali.
Pediatr Infect Dis J. 2021 Sep 1;40(9S):S18-S28. doi: 10.1097/INF.0000000000002767.
We present findings from the Pneumonia Etiology Research for Child Health (PERCH) site in Bamako, Mali.
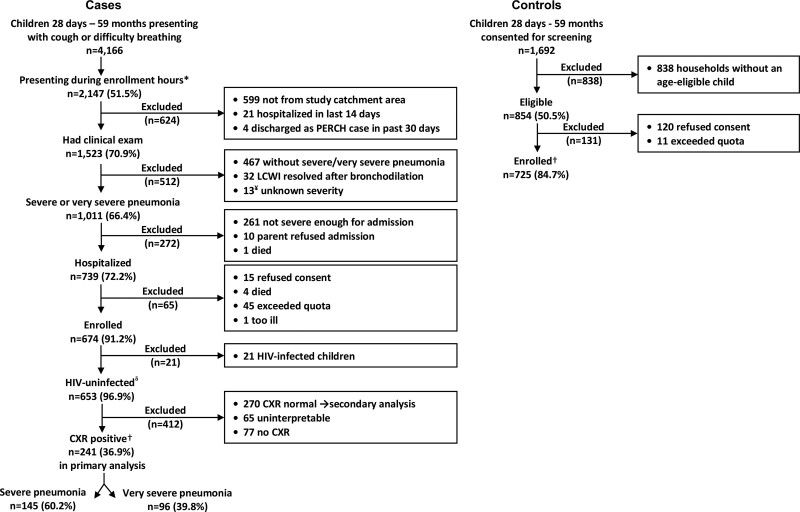
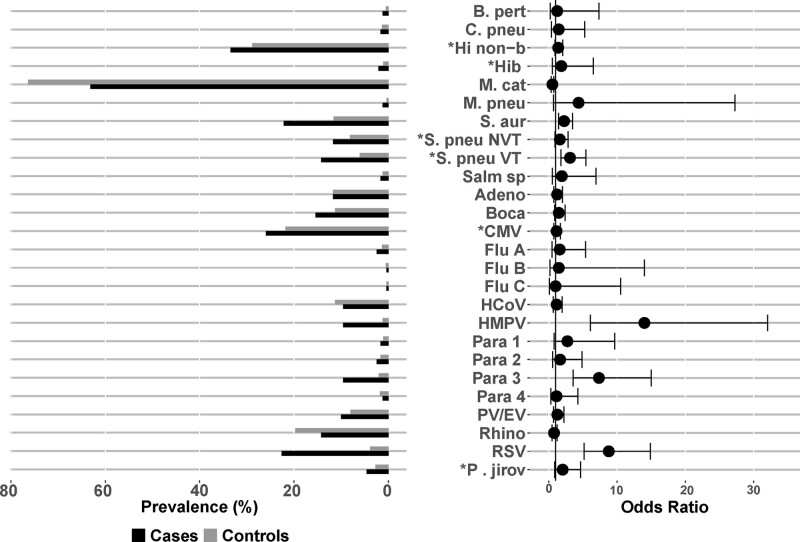
Cases were patients 28 days to 59 months of age, admitted to hospital with severe or very severe pneumonia (2005 World Health Organization definition). Community controls were frequency matched by age. Both provided nasopharyngeal and oropharyngeal swabs for multiplex polymerase chain reaction and Streptococcus pneumoniae culture. Cases underwent blood culture and induced sputum culture for Mycobacterium tuberculosis. A subset had pleural fluid and lung aspirates collected for culture and polymerase chain reaction. Primary analyses included participants with negative or unknown HIV status (HIV-) and cases with abnormal chest radiographs (CXR+). Cases and controls were compared using logistic regression adjusting for age. Etiologic fractions were calculated by a Bayesian nested partially latent class analysis, the PERCH integrated analysis.
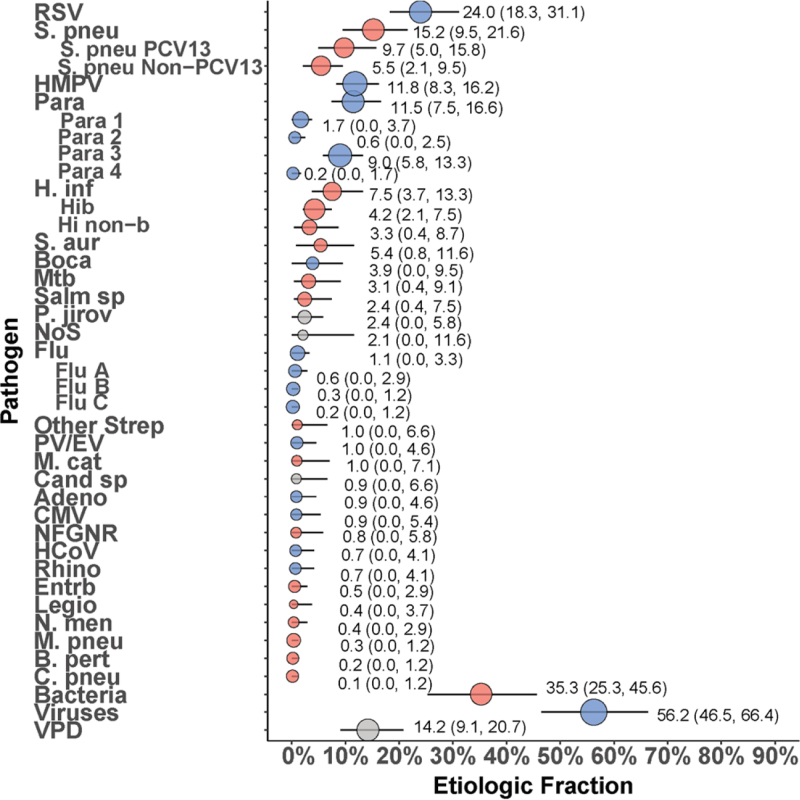
Between January 1, 2012, and January 14, 2014, we enrolled 241 CXR+/HIV- cases and 725 HIV- controls. Compared with controls, cases were more likely to have moderate-to-severe wasting (43.1% vs. 14.1%, P < 0.001) and stunting (26.6% vs. 9.4%, P < 0.001). Predominant etiologies were respiratory syncytial virus [24.0%; 95% credible interval (CrI): 18.3%-31.1%], S. pneumoniae (15.2%; 95% CrI: 9.5-21.6), human metapneumovirus (11.8%; 95% CrI: 8.3%-16.2%) and parainfluenza virus type 3 (9.0%; 95% CrI: 5.8%-13.3%). Case fatality was 13.3%, with Staphylococcus aureus, Pneumocystis jirovecii and Haemophilus influenzae type b predominating (40% of fatal cases).
PERCH uncovered high case fatality among children with severe pneumonia in Mali, highlighting a role for new interventions (eg, respiratory syncytial virus vaccines) and a need to improve vaccine coverage and strengthen healthcare delivery.
我们报告了来自马里巴马科肺炎病因研究儿童健康(PERCH)现场的研究结果。
病例为 28 天至 59 个月龄、因严重或极严重肺炎(2005 年世界卫生组织定义)住院的患者。社区对照病例按年龄频数匹配。两组均采集鼻咽和口咽拭子进行多重聚合酶链反应和肺炎链球菌培养。病例行血培养和诱导痰培养以检测结核分枝杆菌。亚组采集胸腔积液和肺抽吸物进行培养和聚合酶链反应。主要分析包括 HIV 状态为阴性或未知(HIV-)的参与者和胸部 X 线片异常(CXR+)的病例。采用 logistic 回归调整年龄后,对病例和对照进行比较。病因学分率采用贝叶斯嵌套部分潜在类别分析(PERCH 综合分析)进行计算。
2012 年 1 月 1 日至 2014 年 1 月 14 日,我们纳入 241 例 CXR+/HIV-病例和 725 例 HIV-对照。与对照组相比,病例更有可能出现中重度消瘦(43.1%比 14.1%,P<0.001)和发育迟缓(26.6%比 9.4%,P<0.001)。主要病原体包括呼吸道合胞病毒(24.0%;95%可信区间[CrI]:18.3%-31.1%)、肺炎链球菌(15.2%;95% CrI:9.5-21.6)、人偏肺病毒(11.8%;95% CrI:8.3%-16.2%)和副流感病毒 3 型(9.0%;95% CrI:5.8%-13.3%)。病例病死率为 13.3%,金黄色葡萄球菌、卡氏肺孢子虫和乙型流感嗜血杆菌占主导地位(40%的死亡病例)。
PERCH 在马里发现严重肺炎患儿病死率较高,这凸显了新干预措施(如呼吸道合胞病毒疫苗)的作用,需要提高疫苗覆盖率并加强医疗服务。