From the Department of International Health, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland.
International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b).
Pediatr Infect Dis J. 2021 Sep 1;40(9S):S79-S90. doi: 10.1097/INF.0000000000002648.
Pneumonia remains the leading infectious cause of death among children <5 years, but its cause in most children is unknown. We estimated etiology for each child in 2 Bangladesh sites that represent rural and urban South Asian settings with moderate child mortality.
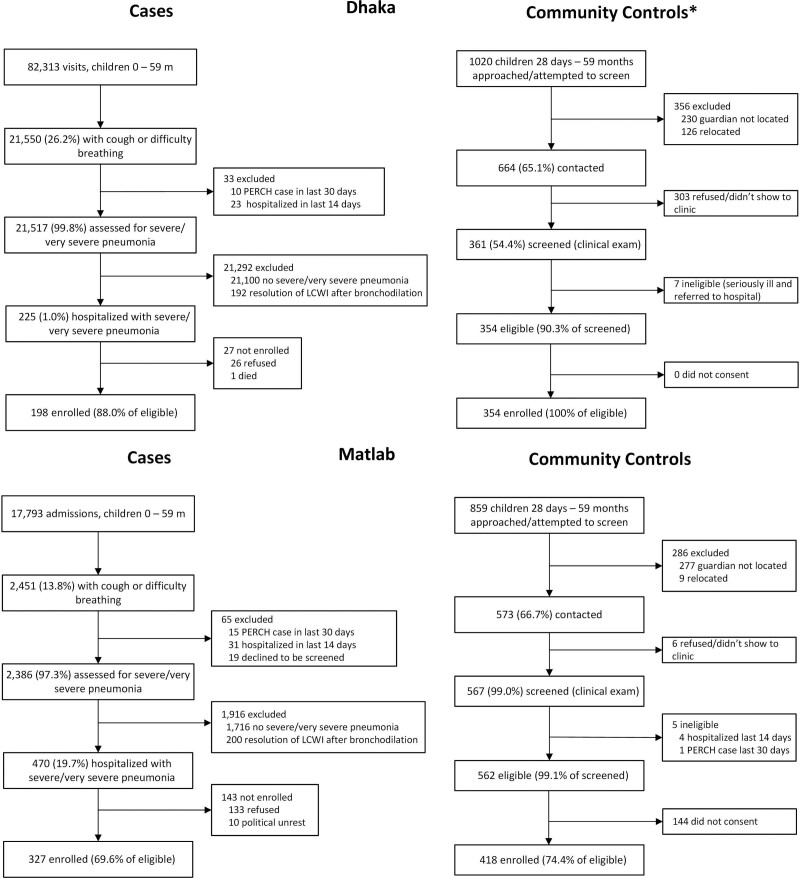
As part of the Pneumonia Etiology Research for Child Health study, we enrolled children 1-59 months of age with World Health Organization-defined severe and very severe pneumonia, plus age-frequency-matched controls, in Matlab and Dhaka, Bangladesh. We applied microbiologic methods to nasopharyngeal/oropharyngeal swabs, blood, induced sputum, gastric and lung aspirates. Etiology was estimated using Bayesian methods that integrated case and control data and accounted for imperfect sensitivity and specificity of the measurements.
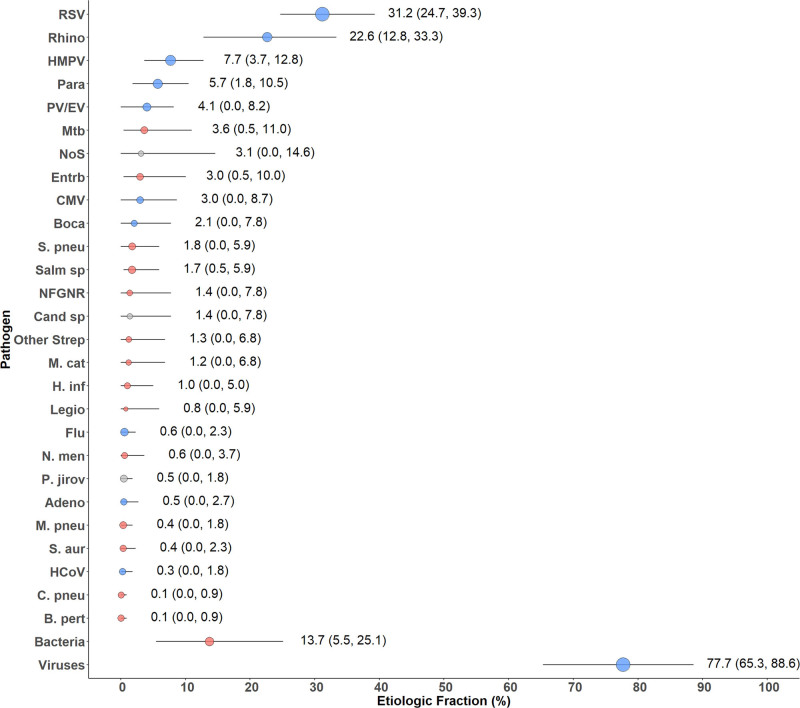
We enrolled 525 cases and 772 controls over 24 months. Of the cases, 9.1% had very severe pneumonia and 42.0% (N = 219) had infiltrates on chest radiograph. Three cases (1.5%) had positive blood cultures (2 Salmonella typhi, 1 Escherichia coli and Klebsiella pneumoniae). All 4 lung aspirates were negative. The etiology among chest radiograph-positive cases was predominantly viral [77.7%, 95% credible interval (CrI): 65.3-88.6], primarily respiratory syncytial virus (31.2%, 95% CrI: 24.7-39.3). Influenza virus had very low estimated etiology (0.6%, 95% CrI: 0.0-2.3). Mycobacterium tuberculosis (3.6%, 95% CrI: 0.5-11.0), Enterobacteriaceae (3.0%, 95% CrI: 0.5-10.0) and Streptococcus pneumoniae (1.8%, 95% CrI: 0.0-5.9) were the only nonviral pathogens in the top 10 etiologies.
Childhood severe and very severe pneumonia in young children in Bangladesh is predominantly viral, notably respiratory syncytial virus.
肺炎仍然是 5 岁以下儿童的主要传染病死因,但大多数儿童的病因不明。我们在孟加拉国的两个地点估计了每个儿童的病因,这两个地点代表了南亚农村和城市地区,儿童死亡率适中。
作为儿童肺炎病因研究的一部分,我们在孟加拉国的 Matlab 和达卡招募了 1-59 个月大的符合世界卫生组织定义的严重和非常严重肺炎的儿童病例,以及年龄匹配的对照儿童。我们应用微生物学方法对鼻咽/口咽拭子、血液、诱导痰、胃和肺抽吸物进行了检测。病因使用贝叶斯方法进行估计,该方法整合了病例和对照数据,并考虑了测量的不完美敏感性和特异性。
我们在 24 个月内招募了 525 例病例和 772 例对照。9.1%的病例为非常严重肺炎,42.0%(N=219)的病例胸部 X 光片有浸润。3 例(1.5%)血培养阳性(2 例伤寒沙门氏菌,1 例大肠埃希菌和肺炎克雷伯菌)。所有 4 例肺抽吸物均为阴性。胸部 X 光片阳性病例的病因主要为病毒[77.7%,95%可信区间(CrI):65.3-88.6],主要为呼吸道合胞病毒(31.2%,95% CrI:24.7-39.3)。流感病毒的估计病因非常低(0.6%,95% CrI:0.0-2.3)。结核分枝杆菌(3.6%,95% CrI:0.5-11.0)、肠杆菌科(3.0%,95% CrI:0.5-10.0)和肺炎链球菌(1.8%,95% CrI:0.0-5.9)是前 10 种病因中唯一的非病毒病原体。
孟加拉国幼儿严重和非常严重肺炎主要为病毒性,尤其是呼吸道合胞病毒。