Departments of Gastroenterology and HepatologyErasmus MC University Medical CenterRotterdamthe Netherlands.
Hepatology. 2022 Feb;75(2):419-429. doi: 10.1002/hep.32131. Epub 2021 Dec 13.
Recently metabolic dysfunction-associated fatty liver disease (MAFLD) has been introduced and was defined as hepatic steatosis with either overweight, diabetes, and/or a combination of other metabolic risk factors. We investigated the application of the MAFLD criteria as compared with NAFLD.
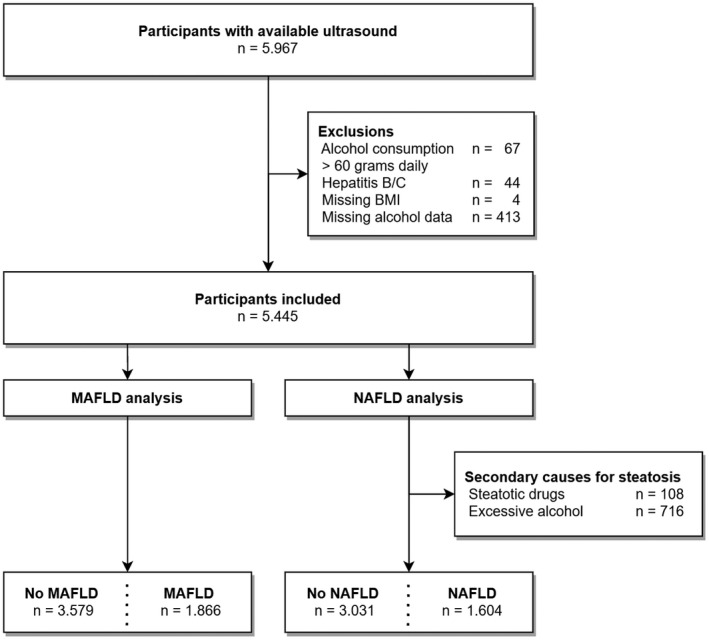
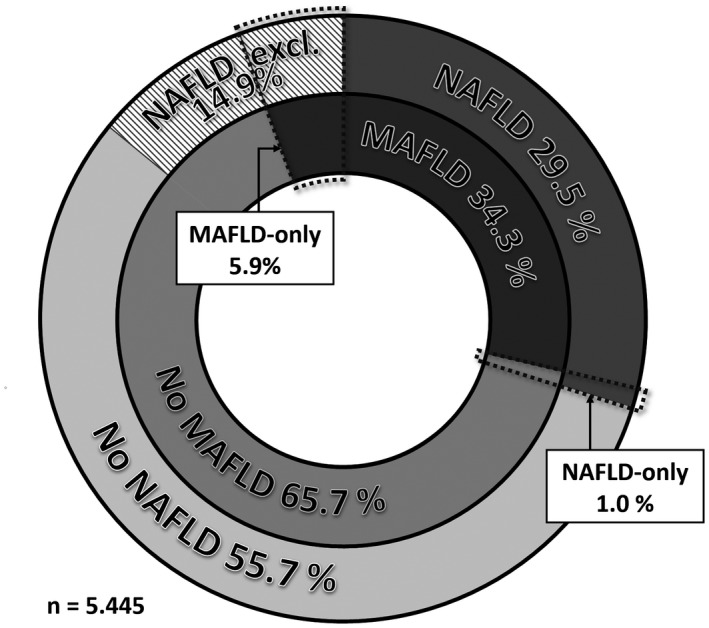
We performed a cross-sectional analysis within the Rotterdam Study, a large prospective population-based cohort. Participants who attended the liver ultrasound and transient elastography program between 2009 and 2014 were eligible for inclusion. Subsequently, individuals with viral hepatitis, alcohol intake >60 g/day, missing alcohol data, and/or missing body mass index were excluded. According to their NAFLD and MAFLD status based on metadata and ultrasound, participants were allocated in overlap fatty liver disease (FLD), NAFLD-only, MAFLD-only, or no FLD. Fibrosis was defined as liver stiffness ≥8.0 kPa. In our analysis, 5445 participants were included: 1866 (34.3%) had MAFLD and 1604 (29.5%) [Correction added on December 27, 2021 after first online publication: The preceding fragment was changed from "1623 (29.8%)"] had NAFLD. This resulted in 1547 (28.4%) [Correction added on December 27, 2021 after first online publication: The preceding fragment was changed from "1566 (28.8%)"] individuals with overlap FLD, 319 (5.9%) [Correction added on December 27, 2021 after first online publication: The preceding fragment was changed from "300 (5.5%)"] with MAFLD-only, 57 (1.0%) with NAFLD-only, and 3522 (64.7%) with no FLD. The MAFLD-only group was strongly associated with fibrosis (adjusted OR 5.30 [Correction added on December 27, 2021 after first online publication: The preceding fragment was changed from "OR 5.27"], p < 0.001) and log-transformed liver stiffness (adjusted beta 0.116, p < 0.001), as opposed to the NAFLD-only group, in which no cases of fibrosis were identified and no association with liver stiffness (adjusted beta 0.006, p = 0.90) was found.
FLD is highly prevalent in the general population. However, not the NAFLD-only, but the MAFLD-only group was associated with fibrosis and higher liver stiffness-independent of demographic and lifestyle factors. We believe that using the MAFLD criteria will help improve the identification and treatment of patients with FLD at risk for fibrosis.
最近提出了代谢相关脂肪性肝病(MAFLD),并将其定义为伴有超重、糖尿病和/或其他代谢危险因素的肝脂肪变性。我们研究了 MAFLD 标准的应用与非酒精性脂肪性肝病(NAFLD)相比的情况。
我们在一项大型前瞻性人群队列 Rotterdam 研究中进行了横断面分析。参加了 2009 年至 2014 年期间的肝脏超声和瞬时弹性成像计划的参与者有资格入选。随后,排除了病毒性肝炎、每日饮酒量>60 g、酒精数据缺失和/或体重指数缺失的个体。根据基于元数据和超声的 NAFLD 和 MAFLD 状态,将参与者分配到重叠性脂肪性肝病(FLD)、单纯性 NAFLD、单纯性 MAFLD 或无 FLD 组。纤维化定义为肝硬度≥8.0 kPa。在我们的分析中,纳入了 5445 名参与者:1866 名(34.3%)患有 MAFLD,1604 名(29.5%)[更正后于 2021 年 12 月 27 日首次在线发布:前一段文字改为“1623 名(29.8%)”]患有 NAFLD。这导致 1547 名(28.4%)[更正后于 2021 年 12 月 27 日首次在线发布:前一段文字改为“1566 名(28.8%)”]重叠性 FLD 患者,319 名(5.9%)[更正后于 2021 年 12 月 27 日首次在线发布:前一段文字改为“300 名(5.5%)”]患有单纯性 MAFLD,57 名(1.0%)患有单纯性 NAFLD,3522 名(64.7%)无 FLD。单纯性 MAFLD 组与纤维化(校正比值比 5.30[更正后于 2021 年 12 月 27 日首次在线发布:前一段文字改为“比值比 5.27”],p<0.001)和肝硬度的自然对数(校正 beta 0.116,p<0.001)呈强烈相关,而单纯性 NAFLD 组则没有纤维化病例,与肝硬度也没有相关性(校正 beta 0.006,p=0.90)。
FLD 在一般人群中患病率很高。然而,与单纯性 NAFLD 相比,只有单纯性 MAFLD 组与纤维化和更高的肝硬度相关,而与人口统计学和生活方式因素无关。我们相信,使用 MAFLD 标准将有助于提高对纤维化风险的 FLD 患者的识别和治疗。