Alhomoud Mohammad, Alhobayb Tamara, Armitage Keith
Division of Hematology and Oncology, Weill Cornell Medical College, New York, NY, USA.
Department of Internal Medicine, University Hospitals Cleveland Medical Center, Cleveland, OH, USA.
IDCases. 2021;26:e01256. doi: 10.1016/j.idcr.2021.e01256. Epub 2021 Aug 24.
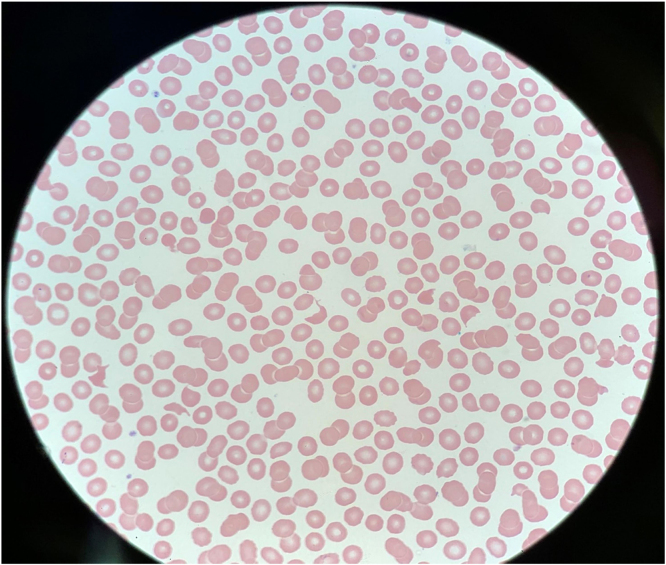
We present a 62-year-old gentleman with history of Crohn's disease, G6PD deficiency, who presented with immune-mediated thrombotic thrombocytopenia purpura (iTTP) one week after the diagnosis of COVID-19 infection. He was admitted with worsening dyspnea, acute renal failure, and profound thrombocytopenia with marked schistocytosis on peripheral smear. ADAMTS13 level was severely deficient. He was treated with oral prednisone, plasma exchange and rituximab with complete clinical resolution. Given the temporal association of this recurrent episode of iTTP with COVID-19 infection and no other discernible cause, COVID-19 infection was the most likely trigger.
我们报告一位62岁男性,有克罗恩病、葡萄糖-6-磷酸脱氢酶(G6PD)缺乏症病史,在诊断为新型冠状病毒肺炎(COVID-19)感染一周后出现免疫介导的血栓性血小板减少性紫癜(iTTP)。他因呼吸困难加重、急性肾衰竭和严重血小板减少伴外周血涂片可见明显裂细胞而入院。ADAMTS13水平严重缺乏。他接受了口服泼尼松、血浆置换和利妥昔单抗治疗,临床症状完全缓解。鉴于此次iTTP复发与COVID-19感染存在时间关联且无其他可识别的病因,COVID-19感染最有可能是触发因素。