Division of Family Planning, Department of Obstetrics, Gynecology and Reproductive Sciences, University of California San Diego, San Diego, CA.
Division of Family Planning, Department of Obstetrics, Gynecology and Reproductive Sciences, University of California San Diego, San Diego, CA.
Am J Obstet Gynecol. 2022 Jan;226(1):95.e1-95.e8. doi: 10.1016/j.ajog.2021.08.028. Epub 2021 Aug 28.
In the United States, up to 57% of women report resumption of sexual activity by the 6 week postpartum visit. Effective contraception should be addressed and provided at that time, to avoid unintended pregnancies and optimize interpregnancy intervals. Long-acting reversible contraceptives are the most effective forms of reversible contraception and are increasingly popular during the postpartum period. However, timing of postpartum intrauterine device (IUD) placement varies among providers and many delay insertion due to concerns for uterine perforation or expulsion of the IUD.
This study aimed to evaluate uterine perforation and expulsion rates with IUD insertion at 4-8 weeks postpartum vs 9-36 weeks postpartum.
We performed a retrospective cohort study using the Kaiser Permanente Southern California electronic medical record from 2010 to 2016. We calculated the proportion of perforations and expulsions with IUD insertion at 4-8 weeks vs 9-36 weeks postpartum. Our primary outcome was the perforation rate. Secondarily, we evaluated the expulsion rate. For our minimum sample size calculation, to detect a difference of 0.5% in the perforation rate, with a baseline perforation rate of 0.5% for the 9-36 week postpartum IUD placement group, 80% power, and 5% alpha error rate, we would need at least 4221 participants per group, 8442 in total.
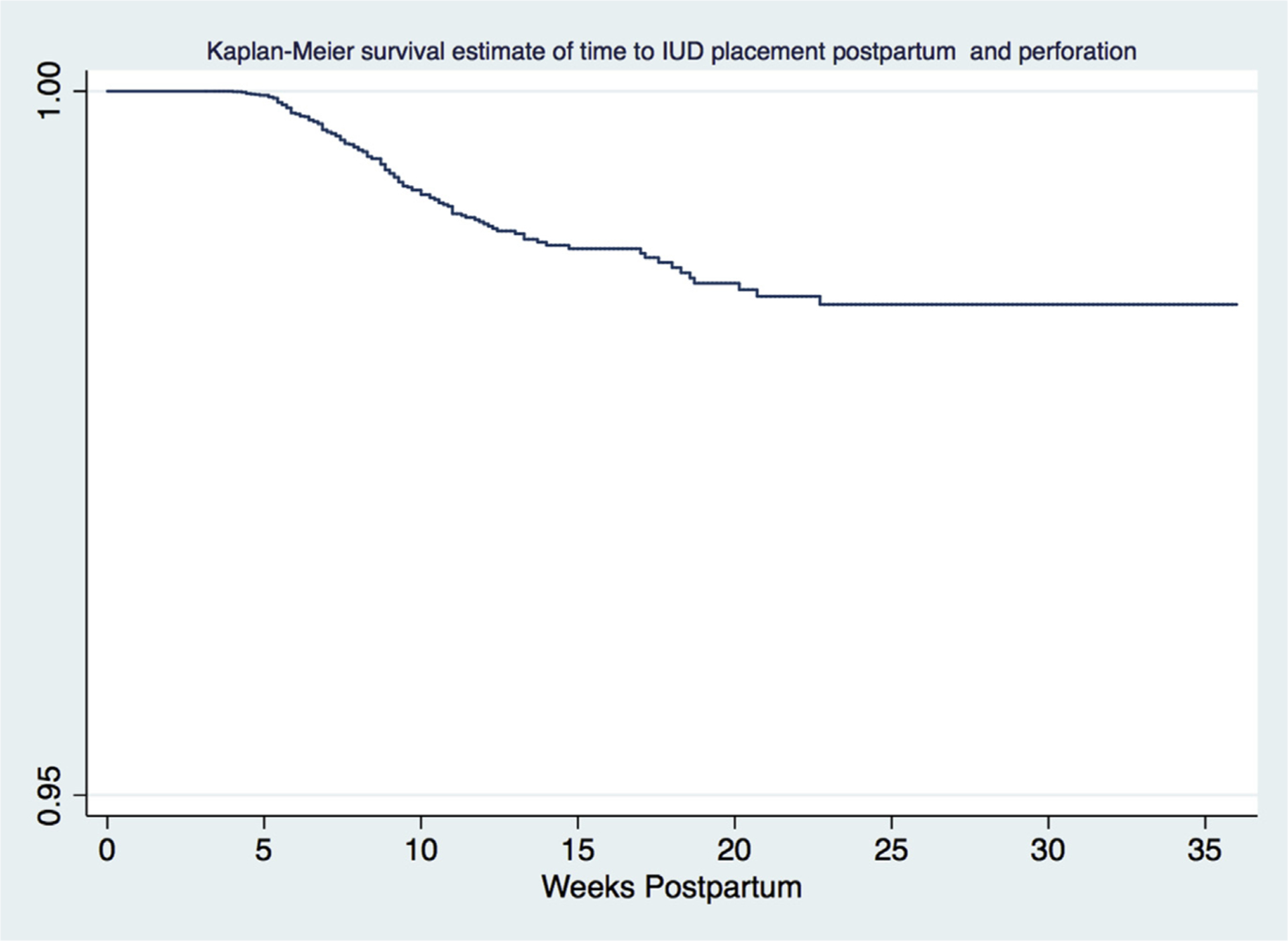
A total of 24,959 patients met inclusion criteria (n=13,180 in the 4-8 week group, n=11,777 in the 9-36 week group). Of 430 patients with a confirmed complication, 157 uterine perforations and 273 IUD expulsions were identified. Perforation rates were significantly higher with placement at 4-8 weeks than at 9-36 weeks (0.78% vs 0.46%; P=.001). After adjusting for race and ethnicity, breastfeeding, IUD type, provider type, parity, most recent delivery, and body mass index, the odds of perforation remained higher with placement at 4-8 weeks than at 9-36 weeks (adjusted odds ratio, 1.92; 95% confidence interval, 1.28-2.89). Our Kaplan-Meier survival curve showed that the risk of uterine perforation remained elevated until approximately 22-23 weeks postpartum. Expulsion rates were similar between the 2 groups (1.02 vs 1.17; P=.52).
Uterine perforation after interval postpartum IUD insertion is greater at 4-8 weeks than at 9-36 weeks, although perforation rates remain low at <1%. Expulsion rates did not differ between the groups. Because overall rates of uterine perforation are low, women can safely be offered IUDs at any interval beyond 4 weeks with minimal concern for perforation.
在美国,多达 57%的女性报告在产后 6 周就诊时恢复了性行为。此时应解决并提供有效的避孕措施,以避免意外怀孕和优化妊娠间隔。长效可逆避孕方法是最有效的可逆避孕方法,在产后期间越来越受欢迎。然而,提供者之间产后宫内节育器(IUD)放置的时间不同,许多人因担心子宫穿孔或 IUD 排出而延迟插入。
本研究旨在评估产后 4-8 周与 9-36 周放置 IUD 的子宫穿孔和排出率。
我们使用 2010 年至 2016 年 Kaiser Permanente 南加州电子病历进行了回顾性队列研究。我们计算了产后 4-8 周与 9-36 周放置 IUD 时穿孔和排出的比例。我们的主要结局是穿孔率。其次,我们评估了排出率。对于我们的最小样本量计算,为了检测 9-36 周产后 IUD 放置组穿孔率 0.5%的差异,基线穿孔率为 0.5%,80%的功率和 5%的 alpha 错误率,我们每组需要至少 4221 名参与者,总共 8442 名参与者。
共有 24959 名患者符合纳入标准(4-8 周组 13180 名,9-36 周组 11777 名)。在 430 名确诊并发症的患者中,发现 157 例子宫穿孔和 273 例 IUD 排出。穿孔率在产后 4-8 周放置时明显高于 9-36 周(0.78%比 0.46%;P=.001)。调整种族和民族、母乳喂养、IUD 类型、提供者类型、产次、最近分娩和体重指数后,4-8 周放置时穿孔的几率仍高于 9-36 周(调整后的优势比,1.92;95%置信区间,1.28-2.89)。我们的 Kaplan-Meier 生存曲线显示,产后 4-8 周子宫穿孔的风险仍然升高,直到大约 22-23 周。两组的排出率相似(1.02 比 1.17;P=.52)。
产后间隔 IUD 插入后子宫穿孔在 4-8 周时大于 9-36 周,尽管穿孔率仍低于 1%。两组的排出率没有差异。由于子宫穿孔的总体发生率较低,因此可以在 4 周后任何时间安全地为女性提供 IUD,而无需过多担心穿孔。