University Clinic for Hematology, Oncology, Hemostaseology and Palliative Care, Johannes Wesling Medical Center Minden, University of Bochum, Hans-Nolte-Straße 1, 32429, Minden, Germany.
Institute of Computational Biology, Helmholtz Center Munich, Ingolstädter Landstraße 1, 85764, Neuherberg, Germany.
Ann Hematol. 2021 Nov;100(11):2707-2716. doi: 10.1007/s00277-021-04647-0. Epub 2021 Aug 31.
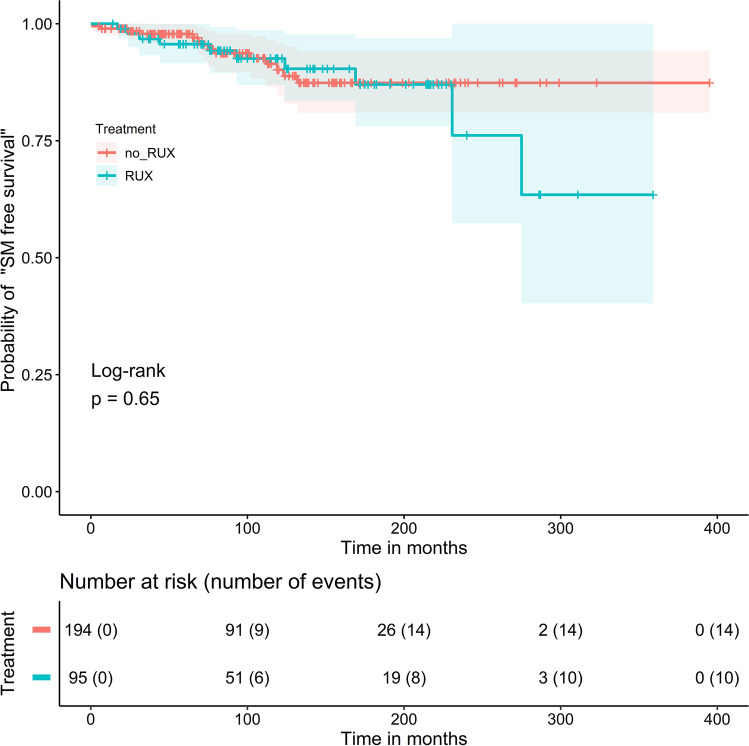
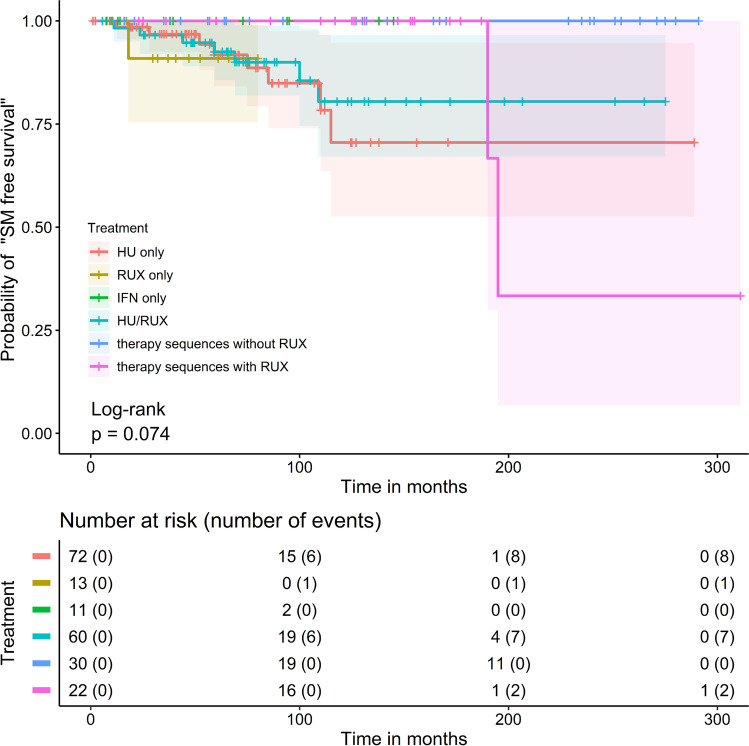
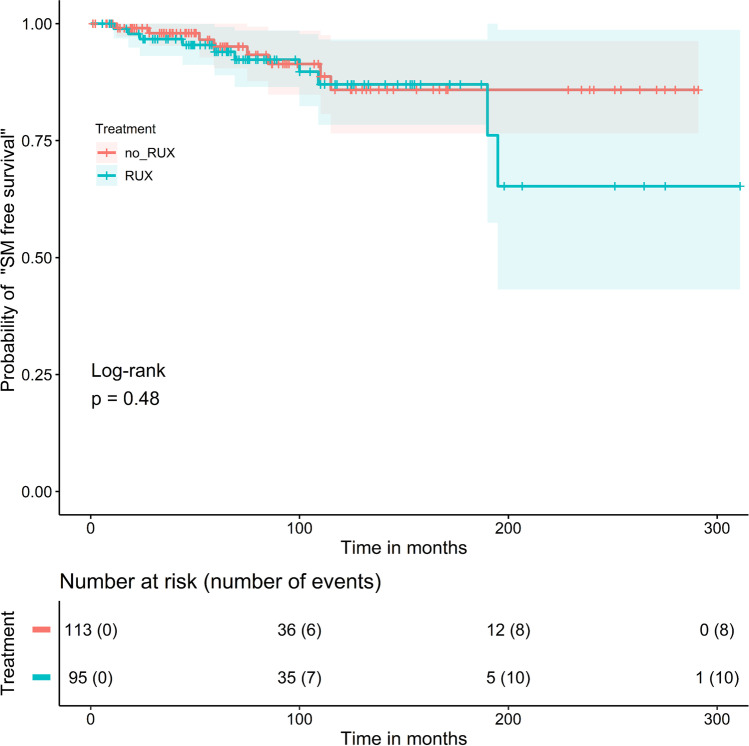
Recently, there has been increased concern about a risk of secondary malignancies (SM) occurring in myelofibrosis (MF) patients receiving ruxolitinib (RUX). In polycythemia vera (PV), on the other hand, only limited data on the risk of SM under RUX treatment are available. To investigate the association between RUX therapy in PV and SM, we conducted a retrospective, single-center study that included 289 PV patients. RUX was administered to 32.9% (95/289) of patients for a median treatment duration of 48.0 months (range 1.0-101.6). Within a median follow-up of 97 months (1.0-395.0) after PV diagnosis, 24 SM occurred. Comparing the number of PV patients with RUX-associated SM (n = 10, 41.7%) with the 14 (58.3%) patients who developed SM without RUX, no significant difference (p = 0.34, chi square test) was found. No increased incidences of melanoma, lymphoma, or solid "non-skin" malignancies were observed with RUX (p = 0.31, p = 0.60, and p = 0.63, respectively, chi square test). However, significantly more NMSC occurred in association with RUX treatment (p = 0.03, chi-squared test). The "SM-free survival" was not significantly different by log rank test for all 289 patients (p = 0.65), for the patients (n = 208; 72%) receiving cytoreductive therapy (p = 0.48) or for different therapy sequences (p = 0.074). In multivariate analysis, advanced age at PV diagnosis (HR 1.062 [95% CI 1.028, 1.098]) but not administration of RUX (HR 1.068 [95% CI 0.468, 2.463]) was associated with an increased risk for SM (p = 0.005). According to this retrospective analysis, no increased risk of SM due to RUX treatment could be substantiated for PV.
最近,人们越来越关注接受鲁索替尼(RUX)治疗的骨髓纤维化(MF)患者发生继发性恶性肿瘤(SM)的风险。另一方面,在真性红细胞增多症(PV)中,只有有限的数据可用于评估 RUX 治疗下 SM 的风险。为了研究 RUX 治疗在 PV 中的应用与 SM 之间的关联,我们进行了一项回顾性、单中心研究,纳入了 289 例 PV 患者。32.9%(95/289)的患者接受了 RUX 治疗,中位治疗时间为 48.0 个月(范围 1.0-101.6)。在 PV 诊断后中位随访 97 个月(1.0-395.0)期间,有 24 例发生 SM。将 10 例(41.7%)发生与 RUX 相关 SM 的 PV 患者与未接受 RUX 治疗但发生 14 例(58.3%)SM 的患者进行比较,未发现差异有统计学意义(p=0.34,卡方检验)。RUX 治疗并未导致黑色素瘤、淋巴瘤或实体“非皮肤”恶性肿瘤的发病率增加(p=0.31,p=0.60 和 p=0.63,卡方检验)。然而,与 RUX 治疗相关的非皮肤恶性肿瘤(NMSC)显著增加(p=0.03,卡方检验)。在所有 289 例患者中,对数秩检验显示“SM 无进展生存”无显著差异(p=0.65);在接受细胞减灭治疗的患者(n=208;72%)中(p=0.48)或在不同的治疗序列中(p=0.074)也未显示出显著差异。在多变量分析中,PV 诊断时年龄较大(HR 1.062 [95%CI 1.028, 1.098]),但不是 RUX 的应用(HR 1.068 [95%CI 0.468, 2.463])与 SM 风险增加相关(p=0.005)。根据这项回顾性分析,RUX 治疗在 PV 中不会增加 SM 的风险。