Department of Systems, Populations, and Leadership, University of Michigan School of Nursing, Ann Arbor.
Department of Biostatistics, Epidemiology, and Informatics, Perelman School of Medicine at the University of Pennsylvania, Philadelphia.
JAMA Netw Open. 2021 Sep 1;4(9):e2122826. doi: 10.1001/jamanetworkopen.2021.22826.
National guidelines recommend against continuous pulse oximetry use for hospitalized children with bronchiolitis who are not receiving supplemental oxygen, yet guideline-discordant use remains high.
To evaluate deimplementation outcomes of educational outreach and audit and feedback strategies aiming to reduce guideline-discordant continuous pulse oximetry use in children hospitalized with bronchiolitis who are not receiving supplemental oxygen.
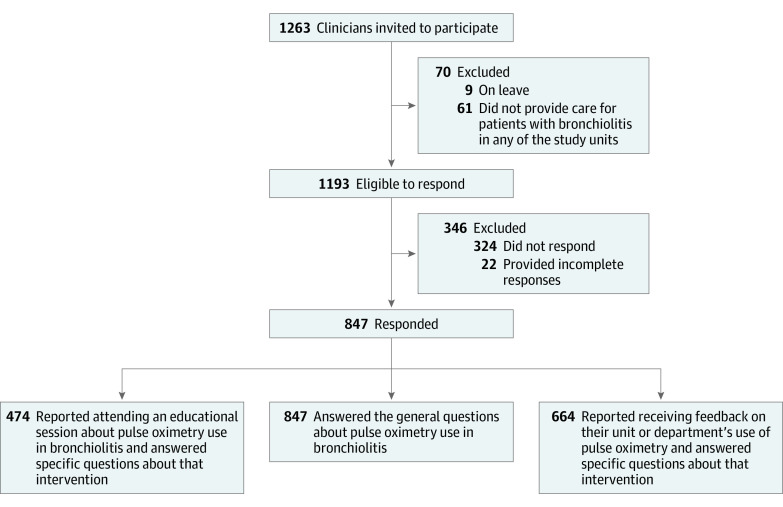
DESIGN, SETTING, AND PARTICIPANTS: A nonrandomized clinical single-group deimplementation trial was conducted in 14 non-intensive care units in 5 freestanding children's hospitals and 1 community hospital from December 1, 2019, through March 14, 2020, among 847 nurses and physicians caring for hospitalized children with bronchiolitis who were not receiving supplemental oxygen.
Educational outreach focused on communicating details of the existing guidelines and evidence. Audit and feedback strategies included 2 formats: (1) weekly aggregate data feedback to multidisciplinary teams with review of unit-level and hospital-level use of continuous pulse oximetry, and (2) real-time 1:1 feedback to clinicians when guideline-discordant continuous pulse oximetry use was discovered during in-person data audits.
Clinician ratings of acceptability, appropriateness, feasibility, and perceived safety were assessed using a questionnaire. Guideline-discordant continuous pulse oximetry use in hospitalized children was measured using direct observation of a convenience sample of patients with bronchiolitis who were not receiving supplemental oxygen.
A total of 847 of 1193 eligible clinicians (695 women [82.1%]) responded to a Likert scale-based questionnaire (71% response rate). Most respondents rated the deimplementation strategies of education and audit and feedback as acceptable (education, 435 of 474 [92%]; audit and feedback, 615 of 664 [93%]), appropriate (education, 457 of 474 [96%]; audit and feedback, 622 of 664 [94%]), feasible (education, 424 of 474 [89%]; audit and feedback, 557 of 664 [84%]), and safe (803 of 847 [95%]). Sites collected 1051 audit observations (range, 47-403 per site) on 709 unique patient admissions (range, 31-251 per site) during a 3.5-month period of continuous pulse oximetry use in children with bronchiolitis not receiving supplemental oxygen, which were compared with 579 observations (range, 57-154 per site) from the same hospitals during the baseline 4-month period (prior season) to determine whether the strategies were associated with a reduction in use. Sites conducted 148 in-person educational outreach and aggregate data feedback sessions and provided real-time 1:1 feedback 171 of 236 times (72% of the time when guideline-discordant monitoring was identified). Adjusted for age, gestational age, time since weaning from supplemental oxygen, and other characteristics, guideline-discordant continuous pulse oximetry use decreased from 53% (95% CI, 49%-57%) to 23% (95% CI, 20%-25%) (P < .001) during the intervention period. There were no adverse events attributable to reduced monitoring.
In this nonrandomized clinical trial, educational outreach and audit and feedback deimplementation strategies for guideline-discordant continuous pulse oximetry use among hospitalized children with bronchiolitis who were not receiving supplemental oxygen were positively associated with clinician perceptions of feasibility, acceptability, appropriateness, and safety. Evaluating the sustainability of deimplementation beyond the intervention period is an essential next step.
ClinicalTrials.gov Identifier: NCT04178941.
国家指南建议对未接受补充氧气的毛细支气管炎住院患儿不连续使用脉搏血氧仪,但仍存在不符合指南的高使用率。
评估教育外展和审核反馈策略的去实施结果,旨在减少未接受补充氧气的毛细支气管炎住院患儿中不符合指南的连续脉搏血氧仪使用。
设计、地点和参与者:一项非随机临床单组去实施试验于 2019 年 12 月 1 日至 2020 年 3 月 14 日在 5 家独立儿童医院和 1 家社区医院的 14 个非重症监护病房进行,涉及 847 名护理人员和医生,他们负责照顾未接受补充氧气的毛细支气管炎住院患儿。
教育外展重点在于传达现有指南和证据的细节。审核反馈策略包括 2 种形式:(1)每周向多学科团队提供汇总数据反馈,同时审查连续脉搏血氧仪的单位和医院使用情况,(2)当发现不符合指南的连续脉搏血氧仪使用时,实时为临床医生提供 1:1 反馈。
使用问卷调查评估临床医生的可接受性、适当性、可行性和感知安全性。使用毛细支气管炎且未接受补充氧气的便利样本患者的直接观察来衡量住院患儿中不符合指南的连续脉搏血氧仪使用情况。
在 1193 名符合条件的临床医生中,共有 847 名(695 名女性[82.1%])回复了基于李克特量表的问卷(71%的回复率)。大多数受访者认为教育和审核反馈策略的去实施是可接受的(教育,474 名中的 435 名[92%];审核反馈,664 名中的 615 名[93%])、适当的(教育,474 名中的 457 名[96%];审核反馈,664 名中的 622 名[94%])、可行的(教育,474 名中的 424 名[89%];审核反馈,664 名中的 557 名[84%])和安全的(847 名中的 803 名[95%])。在 3.5 个月的毛细支气管炎患儿不接受补充氧气期间连续脉搏血氧仪使用期间,各医院共收集了 1051 次审核观察(每个医院范围为 47-403 次),并与同一医院在前一个季节(基础 4 个月)期间的 579 次观察(每个医院范围为 57-154 次)进行比较,以确定这些策略是否与减少使用有关。各医院共进行了 148 次现场教育外展和汇总数据反馈会议,并在 236 次中的 171 次(当发现不符合指南的监测时,72%的时间)提供了实时 1:1 反馈。在干预期间,不符合指南的连续脉搏血氧仪使用率从 53%(95%CI,49%-57%)调整为 23%(95%CI,20%-25%)(P<0.001)。没有因监测减少而导致的不良事件。
在这项非随机临床试验中,针对未接受补充氧气的毛细支气管炎住院患儿的不符合指南的连续脉搏血氧仪使用,教育外展和审核反馈去实施策略与临床医生对可行性、可接受性、适当性和安全性的感知呈正相关。评估干预期后去实施的可持续性是下一步的重要步骤。
ClinicalTrials.gov 标识符:NCT04178941。