Department of Radiology, Charité - Universitätsmedizin Berlin, corporate member of Freie Universität Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health, Charitéplatz 1, 10117, Berlin, Germany.
Data Analytics and Computational Statistics, Hasso Plattner Institute, Digital Engineering Faculty, University of Potsdam, 14482, Potsdam, Germany.
Eur Radiol. 2022 Feb;32(2):1267-1275. doi: 10.1007/s00330-021-08248-3. Epub 2021 Sep 2.
To evaluate the effects of anatomical phantom structure on task-based image quality assessment compared with a uniform phantom background.
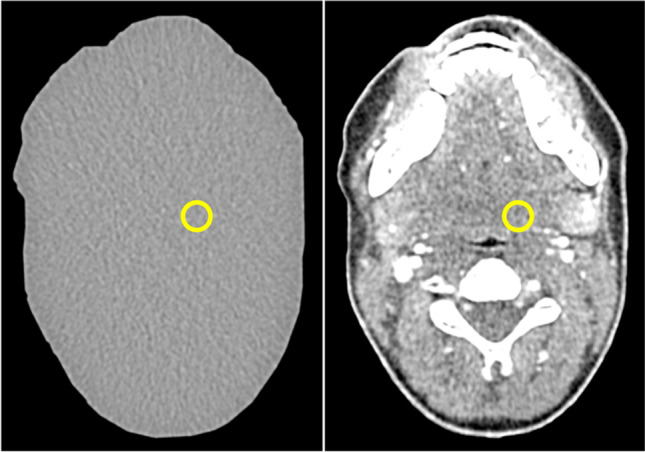
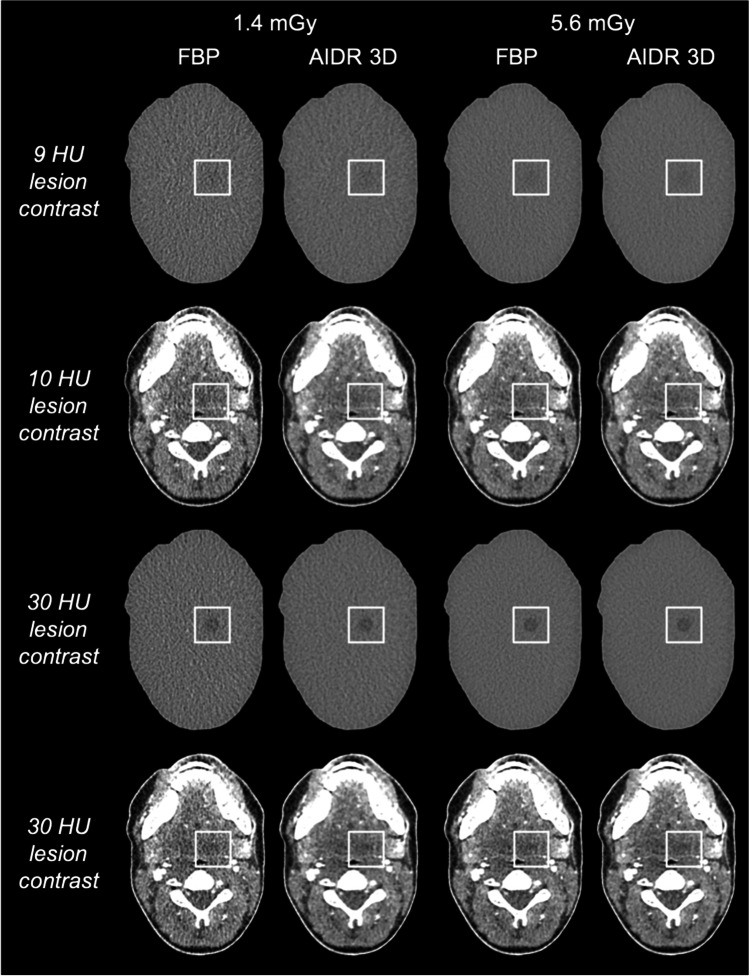
Two neck phantom types of identical shape were investigated: a uniform type containing 10-mm lesions with 4, 9, 18, 30, and 38 HU contrast to the surrounding area and an anatomically realistic type containing lesions of the same size and location with 10, 18, 30, and 38 HU contrast. Phantom images were acquired at two dose levels (CTDIvol of 1.4 and 5.6 mGy) and reconstructed using filtered back projection (FBP) and adaptive iterative dose reduction 3D (AIDR 3D). Detection accuracy was evaluated by seven radiologists in a 4-alternative forced choice experiment.
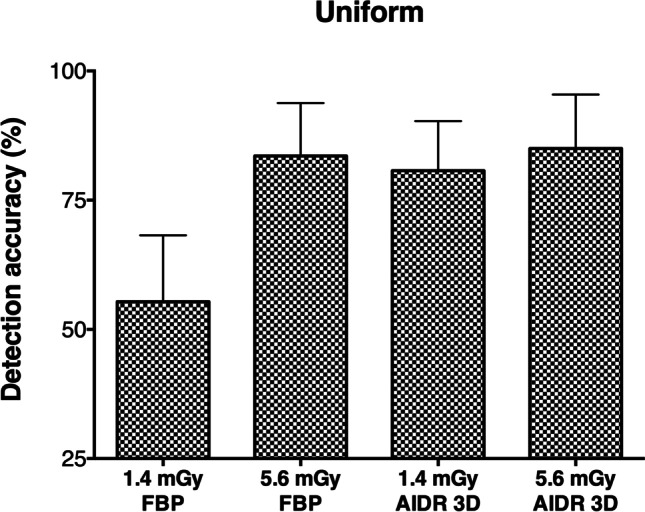
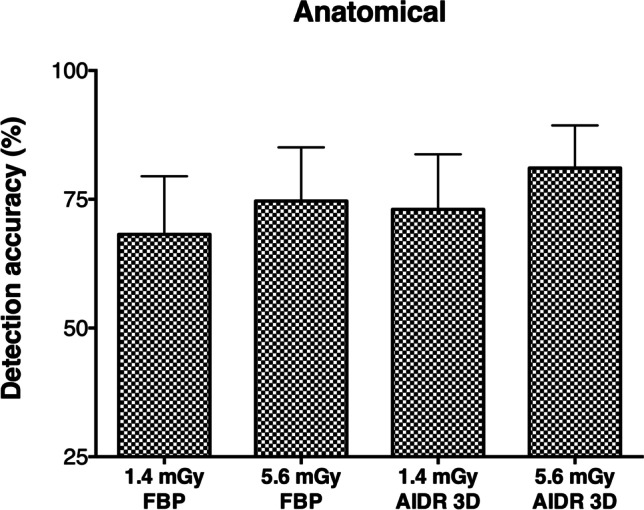
Anatomical phantom structure impaired lesion detection at all lesion contrasts (p < 0.01). Detectability in the anatomical phantom at 30 HU contrast was similar to 9 HU contrast in uniform images (91.1% vs. 89.5%). Detection accuracy decreased from 83.6% at 5.6 mGy to 55.4% at 1.4 mGy in uniform FBP images (p < 0.001), whereas AIDR 3D preserved detectability at 1.4 mGy (80.7% vs. 85% at 5.6 mGy, p = 0.375) and was superior to FBP (p < 0.001). In the assessment of anatomical images, superiority of AIDR 3D was not confirmed and dose reduction moderately affected detectability (74.6% vs. 68.2%, p = 0.027 for FBP and 81.1% vs. 73%, p = 0.018 for AIDR 3D).
A lesion contrast increase from 9 to 30 HU is necessary for similar detectability in anatomical and uniform neck phantom images. Anatomical phantom structure influences task-based assessment of iterative reconstruction and dose effects.
• A lesion contrast increase from 9 to 30 HU is necessary for similar low-contrast detectability in anatomical and uniform neck phantom images. • Phantom background structure influences task-based assessment of iterative reconstruction and dose effects. • Transferability of CT assessment to clinical imaging can be expected to improve as the realism of the test environment increases.
评估解剖体模结构对基于任务的图像质量评估的影响,与均匀体模背景相比。
研究了两种形状相同的颈部体模类型:一种是包含 10-mm 病变的均匀体模,病变与周围区域的对比度为 4、9、18、30 和 38 HU;另一种是包含相同大小和位置病变的解剖逼真体模,病变对比度为 10、18、30 和 38 HU。在两种剂量水平(CTDIvol 为 1.4 和 5.6 mGy)下采集体模图像,并使用滤波反投影(FBP)和自适应迭代剂量降低 3D(AIDR 3D)进行重建。七位放射科医生在 4 项备选强迫选择实验中评估检测准确性。
解剖体模结构降低了所有病变对比度的病变检测(p < 0.01)。在 30 HU 对比度的解剖体模中,检测率与均匀图像中的 9 HU 对比度相似(91.1% vs. 89.5%)。在均匀 FBP 图像中,检测精度从 5.6 mGy 时的 83.6%下降到 1.4 mGy 时的 55.4%(p < 0.001),而 AIDR 3D 在 1.4 mGy 时保持了可检测性(80.7% vs. 5.6 mGy 时的 85%,p = 0.375),优于 FBP(p < 0.001)。在解剖图像评估中,AIDR 3D 的优势并未得到确认,剂量降低适度影响了检测(FBP 为 74.6% vs. 68.2%,p = 0.027,AIDR 3D 为 81.1% vs. 73%,p = 0.018)。
在解剖和均匀颈部体模图像中,病变对比度从 9 增加到 30 HU 是实现相似低对比度检测所必需的。解剖体模结构影响迭代重建和剂量效应的基于任务的评估。
在解剖和均匀颈部体模图像中,病变对比度从 9 增加到 30 HU 是实现相似低对比度检测所必需的。
体模背景结构影响迭代重建和剂量效应的基于任务的评估。
随着测试环境逼真度的提高,预计 CT 评估的临床成像的可转移性将得到改善。