Ma Jiale, Ge Zheng
Department of Hematology, Zhongda Hospital, School of Medicine, Southeast University, Institute of Hematology Southeast University, Nanjing, China.
Department of Hematology, Xuzhou Central Hospital, Xuzhou, China.
Front Pharmacol. 2021 Aug 17;12:701690. doi: 10.3389/fphar.2021.701690. eCollection 2021.
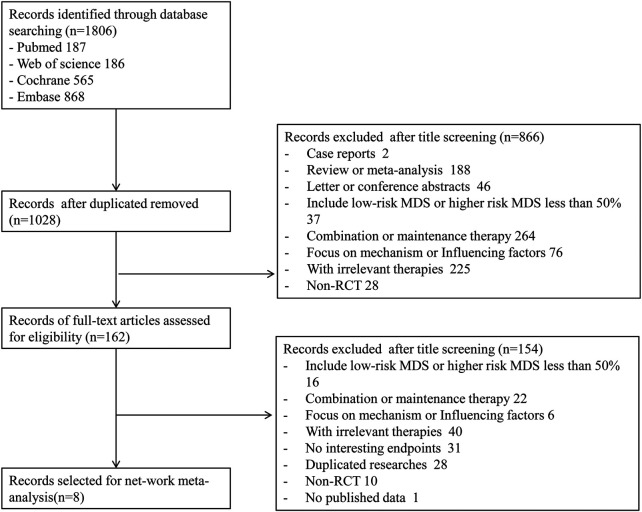
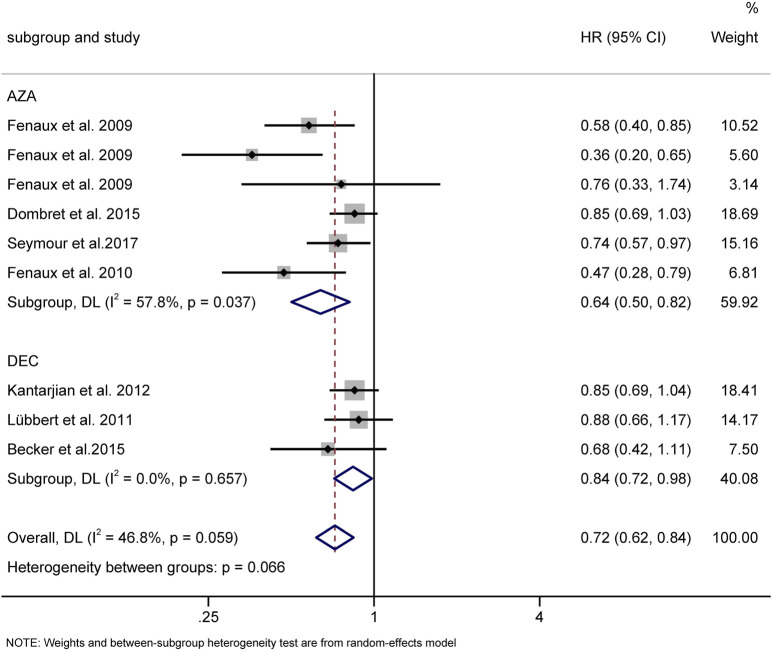
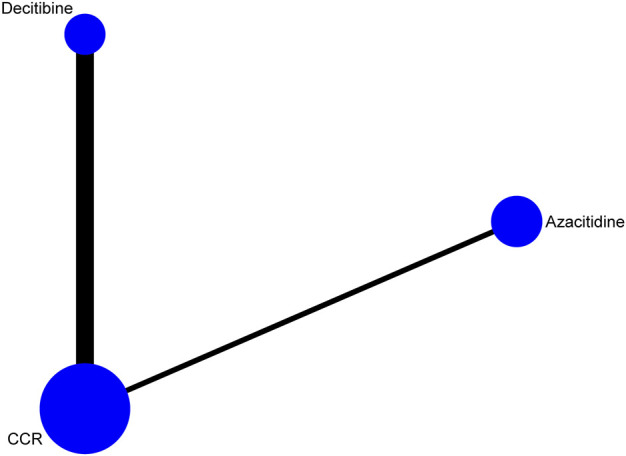
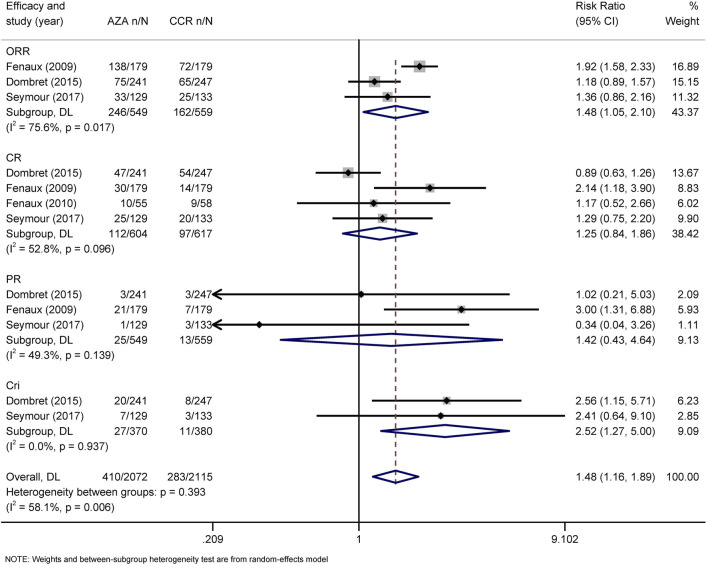
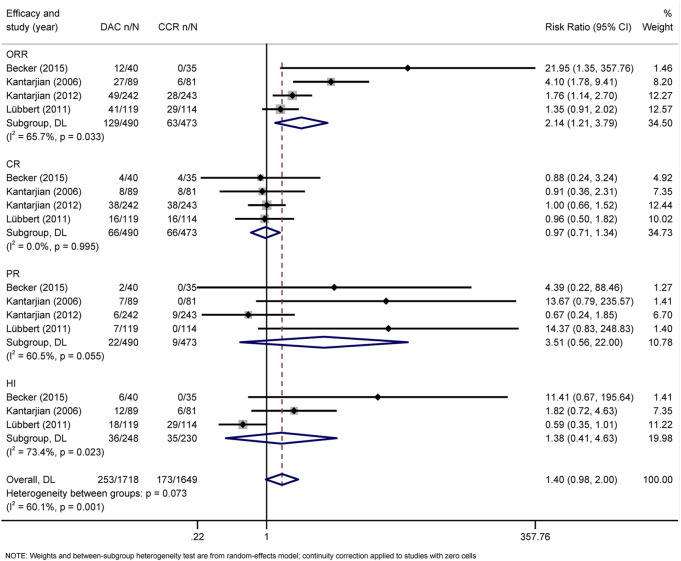
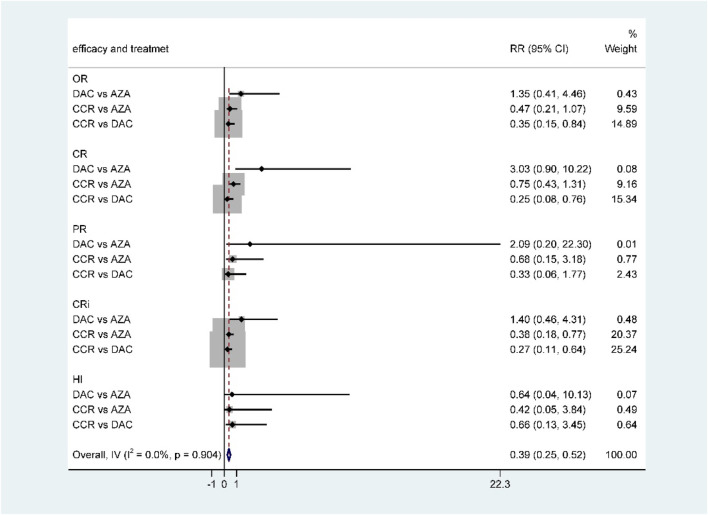
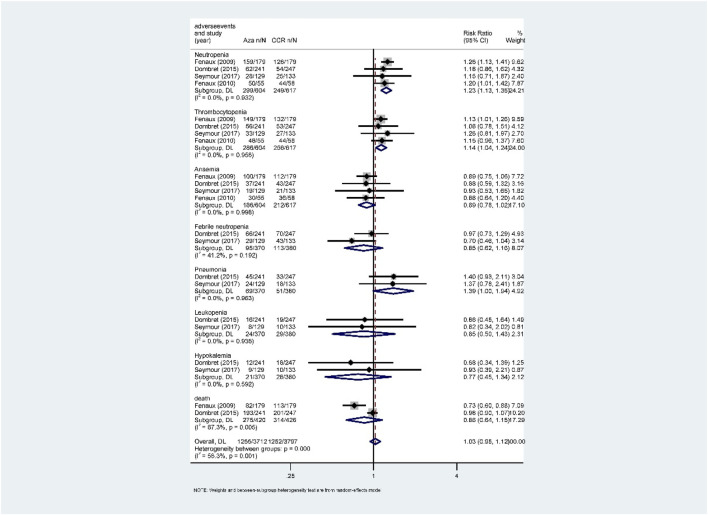
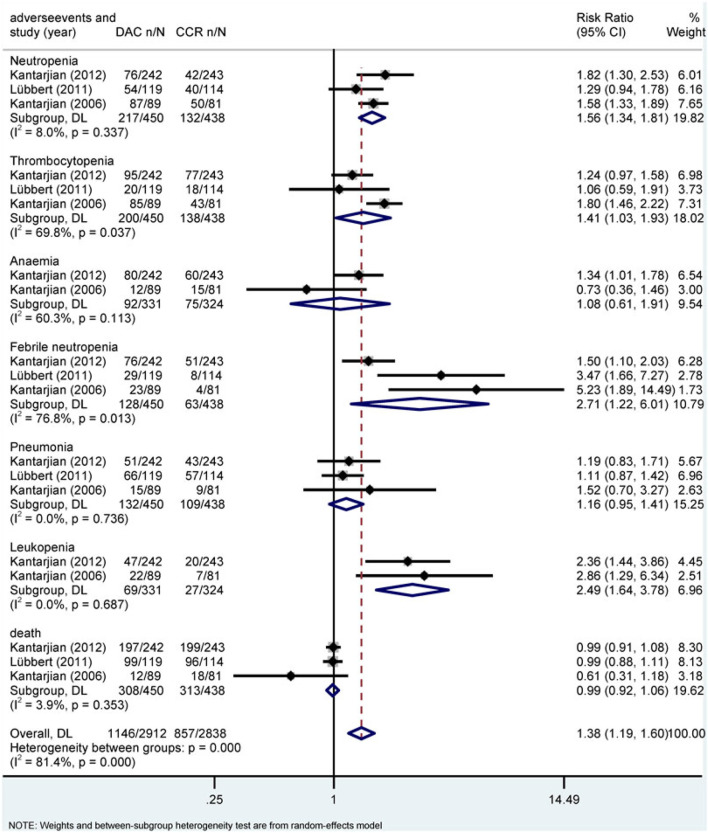
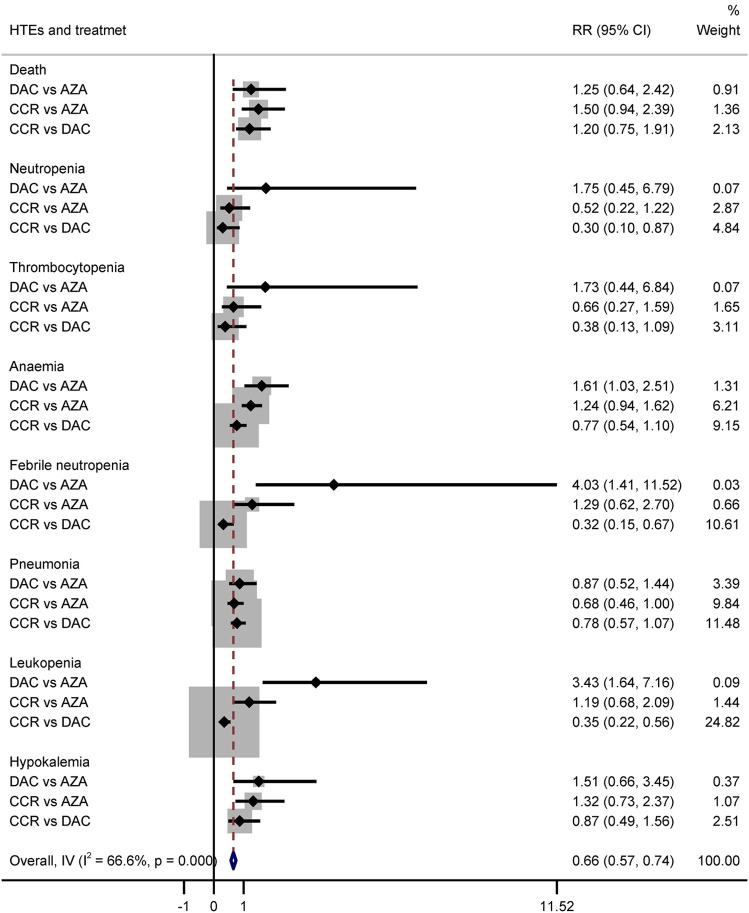
The hypomethylating agents (HMAs) azacitidine (AZA) and decitabine (DAC) have been widely used in patients with acute myeloid leukemia (AML) and higher-risk myelodysplastic syndrome (HR-MDS). However, few direct clinical trials have been carried out to compare the efficacy and adverse events (AEs) between these two agents. The clinical choice between them is controversial. A systematic review and network meta-analysis (NMA) was performed to compare the efficacy, safety, and survival of DAC and AZA in AML and HR-MDS patients. We systematically searched MEDLINE, Embase, Web of Science, and Cochrane Library through March 15, 2021. Randomized controlled trials (RCTs) on AML or HR-MDS patients comparing the efficacy and safety between DAC and AZA or comparing one of HMAs to conventional care regimens (CCR) were selected. Eight RCTs ( = 2,184) were identified in the NMA. Four trials compared AZA to CCR, and four compared DAC to CCR. Direct comparisons indicated that, compared to CCR, both AZA and DAC were associated with higher overall response (OR) rate (AZA vs. CCR: relative risk (RR) = 1.48, 95% CI 1.05-2.1; DAC vs. CCR: RR = 2.14, 95% CI 1.21-3.79) and longer overall survival (OS) (AZA vs. CCR: HR = 0.64, 95% CI 0.50-0.82; DAC vs. CCR: HR = 0.84, 95% CI 0.72-0.98), and AZA showed higher rate of complete remission with incomplete blood count recovery (CRi) (HR = 2.52, 95% CI 1.27-5). For the indirect method, DAC showed a higher complete remission (CR) rate than AZA in patients with both AML (RR = 2.28, 95% CI 1.12-4.65) and MDS (RR = 7.57, 95% CI 1.26-45.54). Additionally, DAC significantly increased the risk of 3/4 grade anemia (RR = 1.61, 95% CI: 1.03-2.51), febrile neutropenia (RR = 4.03, 95% CI: 1.41-11.52), and leukopenia (RR = 3.43, 95% CI 1.64-7.16) compared with AZA. No statistical significance was found for the other studied outcomes. Compared to CCR, both AZA and DAC can promote outcomes in patients with AML and HR-MDS. DAC showed higher efficacy especially CR rate than AZA (low-certainty evidence), while AZA experienced lower frequent grade 3/4 cytopenia than patients receiving DAC treatment.
低甲基化药物(HMAs)阿扎胞苷(AZA)和地西他滨(DAC)已广泛应用于急性髓系白血病(AML)和高危骨髓增生异常综合征(HR-MDS)患者。然而,很少有直接的临床试验来比较这两种药物的疗效和不良事件(AE)。它们之间的临床选择存在争议。进行了一项系统评价和网状Meta分析(NMA),以比较DAC和AZA在AML和HR-MDS患者中的疗效、安全性和生存率。我们通过2021年3月15日对MEDLINE、Embase、科学网和Cochrane图书馆进行了系统检索。选择了关于AML或HR-MDS患者的随机对照试验(RCT),比较DAC和AZA之间的疗效和安全性,或将其中一种HMAs与传统护理方案(CCR)进行比较。在NMA中确定了8项RCT(n = 2184)。4项试验将AZA与CCR进行比较,4项试验将DAC与CCR进行比较。直接比较表明,与CCR相比,AZA和DAC均与更高的总缓解(OR)率相关(AZA与CCR:相对风险(RR)= 1.48,95%CI 1.05 - 2.1;DAC与CCR:RR = 2.14,95%CI 1.21 - 3.79)和更长的总生存期(OS)(AZA与CCR:HR = 0.64,95%CI 0.50 - 0.82;DAC与CCR:HR = 0.84,95%CI 0.72 - 0.98),并且AZA显示出更高的伴有血细胞计数未完全恢复的完全缓解(CRi)率(HR = 2.52,95%CI 1.27 - 5)。对于间接方法,在AML(RR = 2.28,95%CI 1.12 - 4.65)和MDS(RR = 7.57,95%CI 1.26 - 45.54)患者中,DAC显示出比AZA更高的完全缓解(CR)率。此外,与AZA相比,DAC显著增加了3/4级贫血(RR = 1.61,95%CI:1.03 - 2.51)、发热性中性粒细胞减少(RR = 4.03,95%CI:1.41 - 11.52)和白细胞减少(RR = 3.43,95%CI 1.64 - 7.16)的风险。其他研究结果未发现统计学意义。与CCR相比,AZA和DAC均可改善AML和HR-MDS患者的预后。DAC显示出比AZA更高的疗效,尤其是CR率(低确定性证据),而接受AZA治疗的患者3/4级血细胞减少的频率低于接受DAC治疗的患者。