ImmunoConcEpt, CNRS, UMR 5164, University of Bordeaux, Bordeaux, France.
Rheumatology Department, CHU Bordeaux Hospital, Bordeaux, France.
Clin Rev Allergy Immunol. 2023 Jun;64(3):262-283. doi: 10.1007/s12016-021-08889-8. Epub 2021 Sep 6.
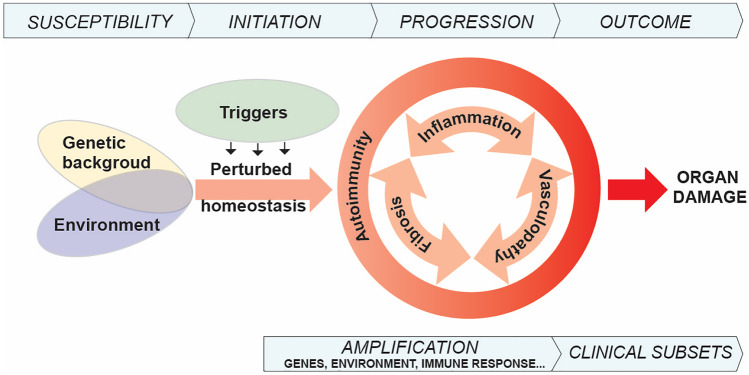
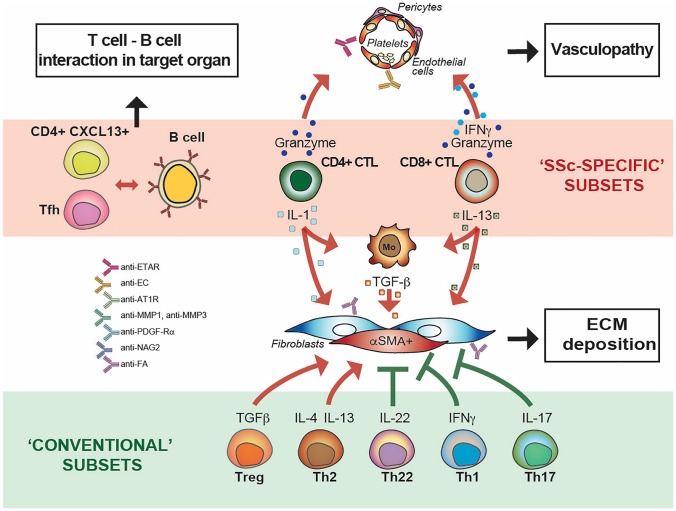
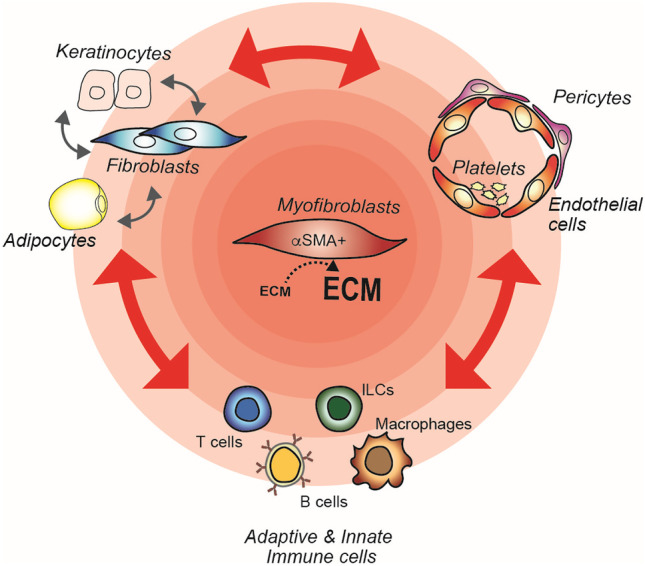
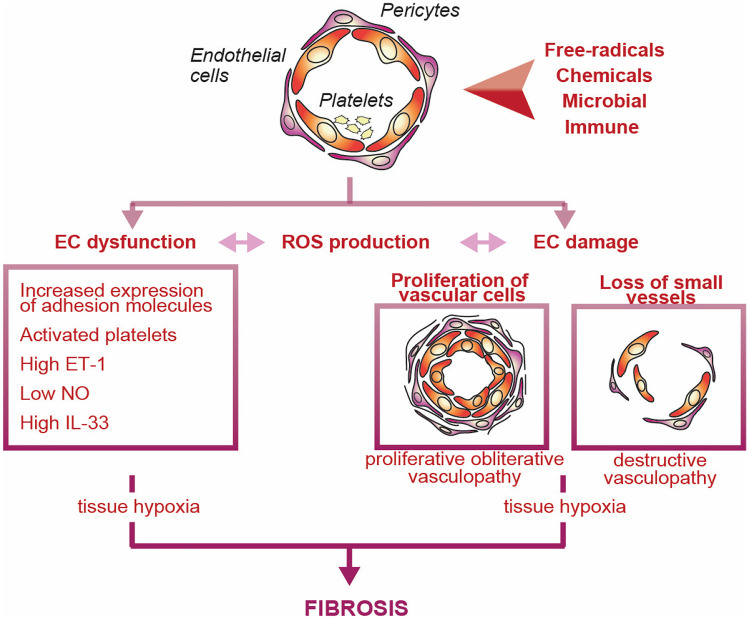
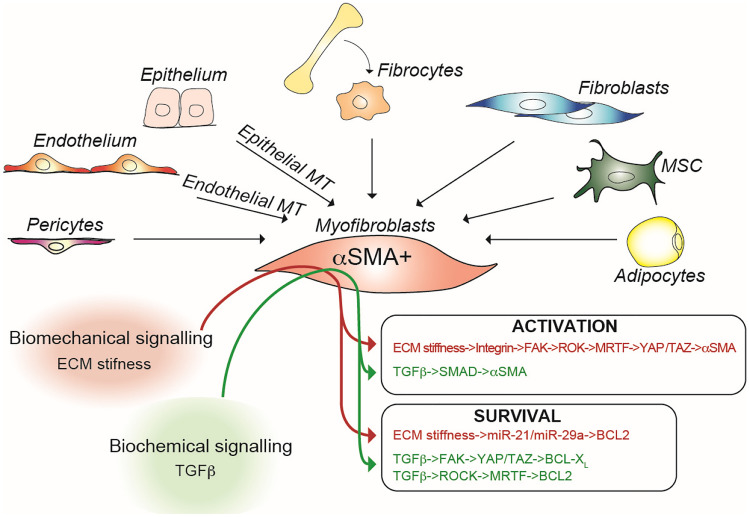
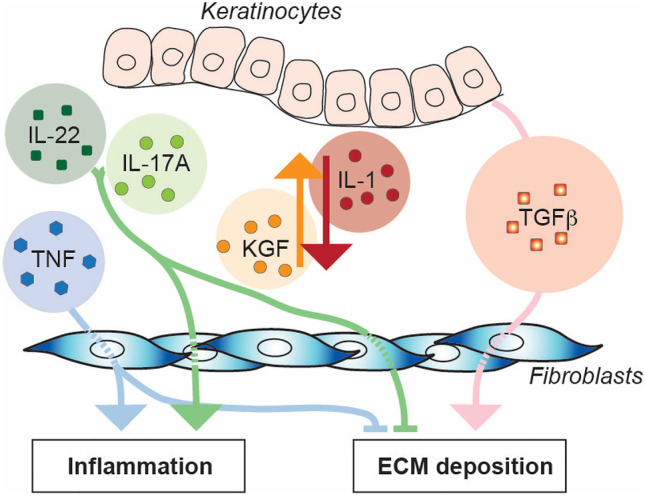
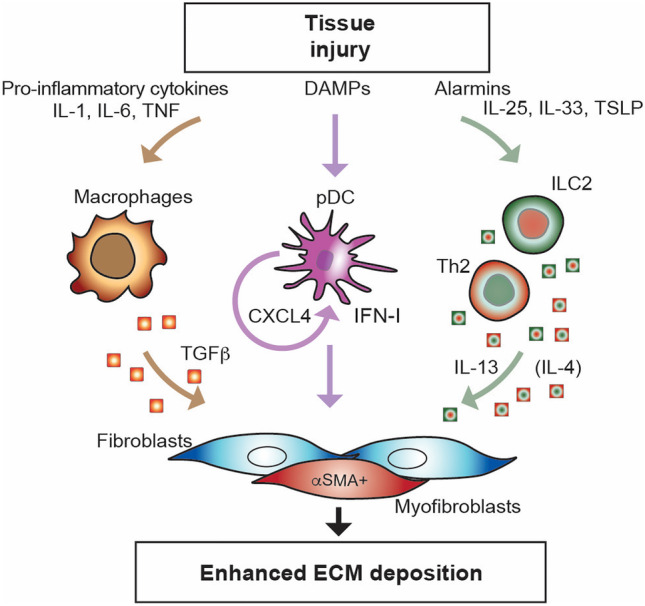
From the clinical standpoint, systemic sclerosis (SSc) is characterized by skin and internal organ fibrosis, diffuse fibroproliferative vascular modifications, and autoimmunity. Clinical presentation and course are highly heterogenous and life expectancy variably affected mostly dependent on lung and heart involvement. SSc touches more women than men with differences in disease severity and environmental exposure. Pathogenetic events originate from altered homeostasis favored by genetic predisposition, environmental cues and a variety of endogenous and exogenous triggers. Epigenetic modifications modulate SSc pathogenesis which strikingly associate profound immune-inflammatory dysregulation, abnormal endothelial cell behavior, and cell trans-differentiation into myofibroblasts. SSc myofibroblasts show enhanced survival and enhanced extracellular matrix deposition presenting altered structure and altered physicochemical properties. Additional cell types of likely pathogenic importance are pericytes, platelets, and keratinocytes in conjunction with their relationship with vessel wall cells and fibroblasts. In SSc, the profibrotic milieu is favored by cell signaling initiated in the one hand by transforming growth factor-beta and related cytokines and in the other hand by innate and adaptive type 2 immune responses. Radical oxygen species and invariant receptors sensing danger participate to altered cell behavior. Conventional and SSc-specific T cell subsets modulate both fibroblasts as well as endothelial cell dysfunction. Beside autoantibodies directed against ubiquitous antigens important for enhanced clinical classification, antigen-specific agonistic autoantibodies may have a pathogenic role. Recent studies based on single-cell RNAseq and multi-omics approaches are revealing unforeseen heterogeneity in SSc cell differentiation and functional states. Advances in system biology applied to the wealth of data generated by unbiased screening are allowing to subgroup patients based on distinct pathogenic mechanisms. Deciphering heterogeneity in pathogenic mechanisms will pave the way to highly needed personalized therapeutic approaches.
从临床角度来看,系统性硬化症 (SSc) 的特征是皮肤和内脏器官纤维化、弥漫性纤维增生性血管改变和自身免疫。临床表现和病程高度异质,预期寿命受肺部和心脏受累的影响各不相同。SSc 影响的女性多于男性,疾病严重程度和环境暴露存在差异。发病机制源于遗传易感性、环境线索和多种内源性和外源性触发因素改变的内稳态。表观遗传修饰调节 SSc 的发病机制,强烈关联到深刻的免疫炎症失调、异常的内皮细胞行为和细胞向肌成纤维细胞的转化。SSc 肌成纤维细胞表现出增强的生存能力和增强的细胞外基质沉积,呈现出改变的结构和改变的物理化学特性。可能具有致病重要性的其他细胞类型是周细胞、血小板和角质形成细胞,以及它们与血管壁细胞和成纤维细胞的关系。在 SSc 中,促纤维化微环境有利于一方面由转化生长因子-β和相关细胞因子启动的细胞信号转导,另一方面由固有和适应性 2 型免疫反应启动的细胞信号转导。活性氧和识别危险的不变受体参与改变细胞行为。传统和 SSc 特异性 T 细胞亚群调节成纤维细胞和内皮细胞功能障碍。除了针对普遍存在的抗原的自身抗体,这些抗原对增强临床分类很重要外,抗原特异性激动性自身抗体可能具有致病作用。基于单细胞 RNAseq 和多组学方法的最近研究揭示了 SSc 细胞分化和功能状态的意想不到的异质性。系统生物学的进展应用于无偏筛选产生的大量数据,允许根据不同的致病机制对患者进行分组。解析致病机制的异质性将为急需的个性化治疗方法铺平道路。