Department of Medical Oncology and Therapeutics Research, City of Hope Comprehensive Cancer Center, Duarte, CA.
Dana-Farber Cancer Institute, Harvard Medical School, Boston, MA.
J Clin Oncol. 2021 Nov 20;39(33):3725-3736. doi: 10.1200/JCO.21.00939. Epub 2021 Sep 7.
COSMIC-021 is evaluating cabozantinib plus atezolizumab in patients with solid tumors. We report results from patients with advanced clear cell (cc) and non-clear cell (ncc) renal cell carcinoma (RCC).
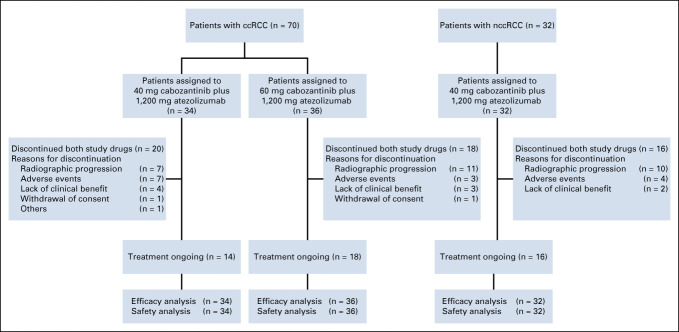
This phase Ib study (NCT03170960) enrolled patients age ≥ 18 years with advanced RCC. A dose-escalation stage was followed by expansion cohorts. For cohort expansion, prior systemic therapy was not permitted for ccRCC but allowed for nccRCC. Patients received oral cabozantinib 40 mg once a day (ccRCC and nccRCC) or 60 mg once a day (ccRCC only) plus atezolizumab (1,200 mg intravenously, once every 3 weeks). The primary end point was investigator-assessed objective response rate (ORR) per RECIST v1.1; the secondary end point was safety.
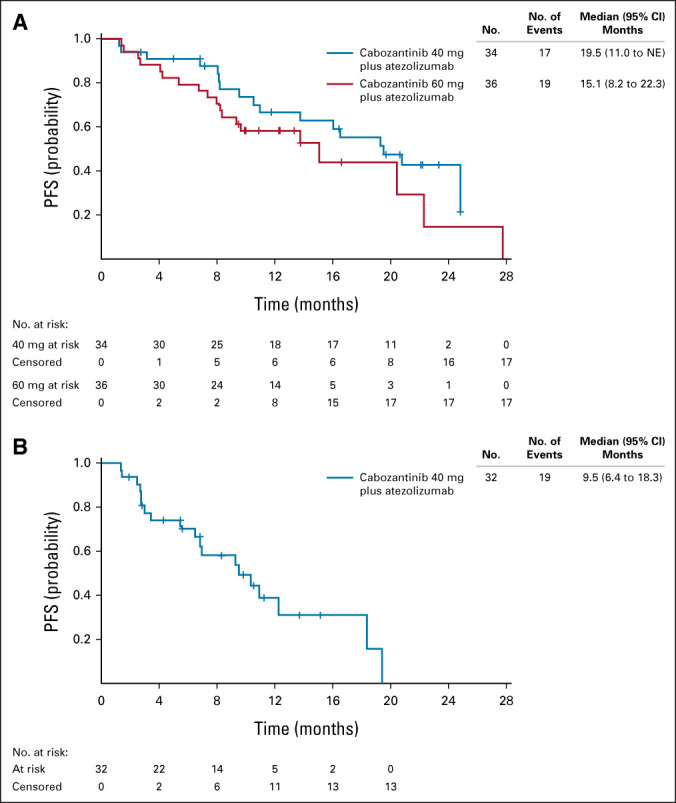
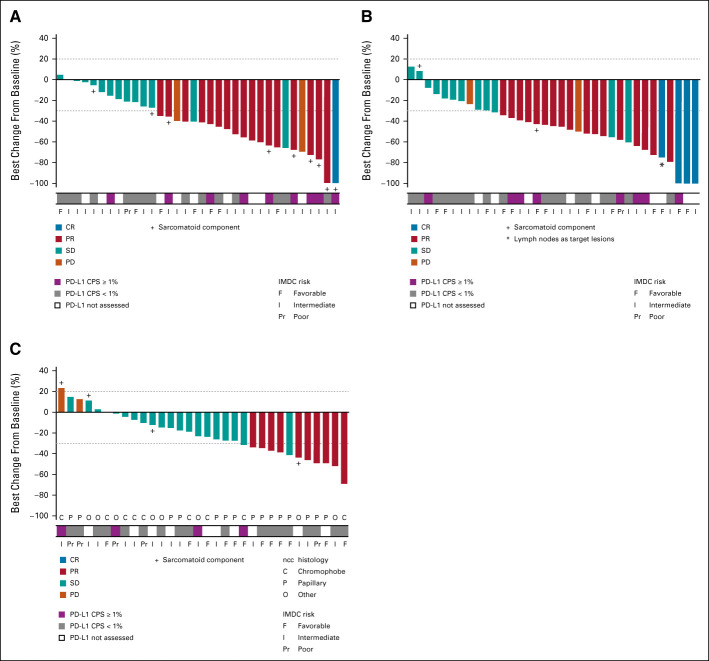
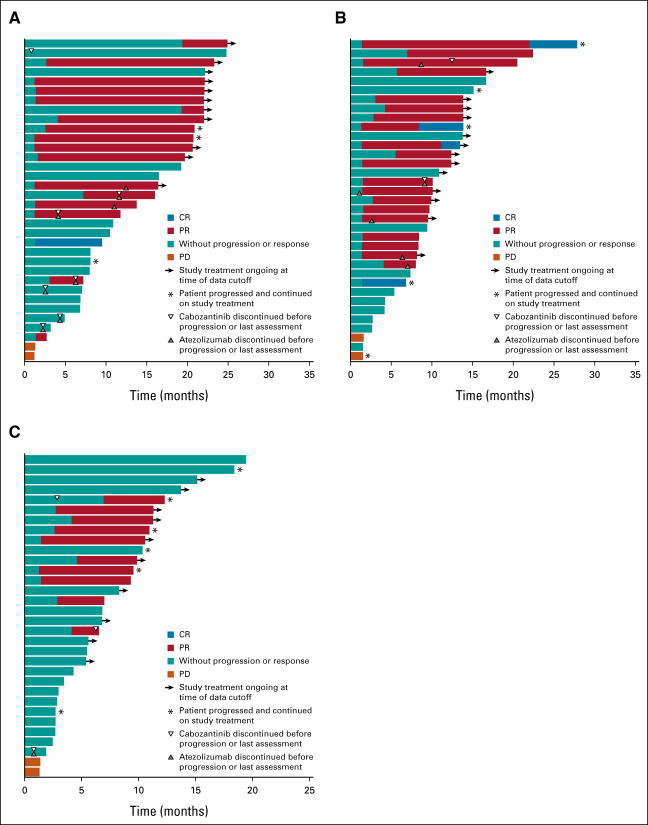
A total of 102 patients were enrolled. Median follow-up was 25.8, 15.3, and 13.3 months for the 40-mg ccRCC, 60-mg ccRCC, and nccRCC groups, respectively. ORR was 53% (80% CI, 41 to 65) in the 40-mg ccRCC group (n = 34) and 58% (80% CI, 46 to 70) in the 60-mg ccRCC group (n = 36), 3% and 11%, respectively, with complete response; median progression-free survival (exploratory end point) was 19.5 and 15.1 months, respectively. In nccRCC (n = 32), ORR was 31% (80% CI, 20 to 44), all partial responses; median progression-free survival was 9.5 months. Grade 3 or 4 treatment-related adverse events (TRAEs) were reported by 71% of patients in the 40-mg ccRCC group, 67% in the 60-mg ccRCC group, and 38% in the nccRCC group; TRAEs leading to discontinuation of both agents occurred in 15%, 6%, and 3% of patients, respectively. There were no grade 5 TRAEs.
The novel combination of cabozantinib plus atezolizumab demonstrated encouraging clinical activity and acceptable tolerability in patients with advanced ccRCC and nccRCC. Disease control was observed across dose levels and histologic subtypes.
COSMIC-021 评估卡博替尼联合阿替利珠单抗在实体瘤患者中的疗效。我们报告了晚期透明细胞(cc)和非透明细胞(ncc)肾细胞癌(RCC)患者的结果。
这是一项 I 期 Ib 研究(NCT03170960),纳入了年龄≥18 岁的晚期 RCC 患者。首先进行剂量递增阶段,然后进行扩展队列研究。对于扩展队列,ccRCC 患者既往不允许接受系统治疗,但 nccRCC 患者允许接受系统治疗。患者接受卡博替尼 40 mg 口服,每日一次(ccRCC 和 nccRCC)或 60 mg 口服,每日一次(仅用于 ccRCC),联合阿替利珠单抗(1200 mg 静脉注射,每 3 周一次)。主要终点为研究者评估的客观缓解率(ORR)根据 RECIST v1.1 标准;次要终点为安全性。
共纳入 102 例患者。40-mg ccRCC 组、60-mg ccRCC 组和 nccRCC 组的中位随访时间分别为 25.8、15.3 和 13.3 个月。40-mg ccRCC 组的 ORR 为 53%(80%CI,41 至 65)(n=34),60-mg ccRCC 组为 58%(80%CI,46 至 70)(n=36),分别有 3%和 11%的患者完全缓解;中位无进展生存期(探索性终点)分别为 19.5 个月和 15.1 个月。nccRCC 组(n=32)的 ORR 为 31%(80%CI,20 至 44),均为部分缓解;中位无进展生存期为 9.5 个月。40-mg ccRCC 组、60-mg ccRCC 组和 nccRCC 组分别有 71%、67%和 38%的患者发生 3 级或 4 级治疗相关不良事件(TRAEs);分别有 15%、6%和 3%的患者因 TRAEs 而停止使用两种药物。无 5 级 TRAEs。
卡博替尼联合阿替利珠单抗在晚期 ccRCC 和 nccRCC 患者中显示出令人鼓舞的临床活性和可接受的耐受性。在不同剂量水平和组织学亚型中观察到疾病控制。