Shaffer Andrew, Rahn Elizabeth, Saag Kenneth, Mudano Amy, Gaffo Angelo
Division of Rheumatology, University of Utah, 30 N 1900 E, SOM4B200, Salt Lake City, UT, 84132, USA.
Division of Rheumatology, University of Alabama at Birmingham, SHEL 306 1530 3rd Ave S, Birmingham, AL, 35294, USA.
BMC Rheumatol. 2021 Sep 8;5(1):32. doi: 10.1186/s41927-021-00202-6.
Previous studies have noted significant variation in serum urate (sUA) levels, and it is unknown how this influences the accuracy of hyperuricemia classification based on single data points. Despite this known variability, hyperuricemic patients are often used as a control group in gout studies. Our objective was to determine the accuracy of hyperuricemia classifications based on single data points versus multiple data points given the degree of variability observed with serial measurements of sUA.
Data was analyzed from a cross-over clinical trial of urate-lowering therapy in young adults without a gout diagnosis. In the control phase, sUA levels used for this analysis were collected at 2-4 week intervals. Mean coefficient of variation for sUA was determined, as were rates of conversion between normouricemia (sUA ≤6.8 mg/dL) and hyperuricemia (sUA > 6.8 mg/dL).
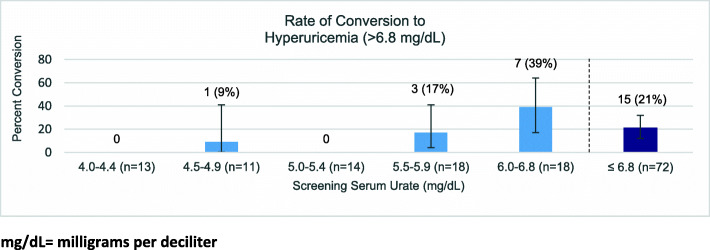
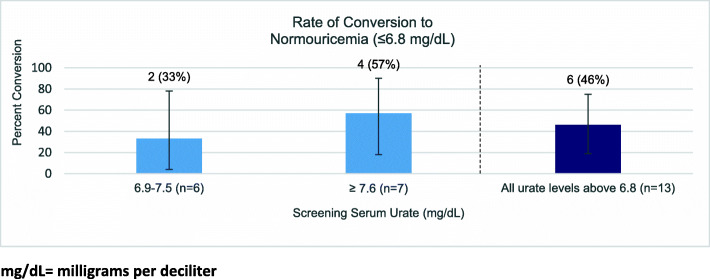
Mean study participant (n = 85) age was 27.8 ± 7.0 years, with 39% female participants and 41% African-American participants. Mean sUA coefficient of variation was 8.5% ± 4.9% (1 to 23%). There was no significant difference in variation between men and women, or between participants initially normouricemic and those who were initially hyperuricemic. Among those initially normouricemic (n = 72), 21% converted to hyperuricemia during at least one subsequent measurement. The subgroup with initial sUA < 6.0 (n = 54) was much less likely to have future values in the range of hyperuricemia compared to the group with screening sUA values between 6.0-6.8 (n = 18) (7% vs 39%, p = 0.0037). Of the participants initially hyperuricemic (n = 13), 46% were later normouricemic during at least one measurement.
Single sUA measurements were unreliable in hyperuricemia classification due to spontaneous variation. Knowing this, if a single measurement must be used in classification, it is worth noting that those with an sUA of < 6.0 mg/dL were less likely to demonstrate future hyperuricemic measurements and this could be considered a safer threshold to rule out intermittent hyperuricemia based on a single measurement point.
Data from parent study ClinicalTrials.gov Identifier: NCT02038179 .
既往研究已注意到血清尿酸(sUA)水平存在显著差异,而尚不清楚这如何影响基于单个数据点的高尿酸血症分类的准确性。尽管存在这种已知的变异性,但高尿酸血症患者在痛风研究中常被用作对照组。我们的目的是根据sUA系列测量所观察到的变异性程度,确定基于单个数据点与多个数据点的高尿酸血症分类的准确性。
对一项针对未诊断为痛风的年轻人进行的降尿酸治疗的交叉临床试验数据进行分析。在对照阶段,每隔2 - 4周收集用于该分析的sUA水平。确定sUA的平均变异系数,以及正常尿酸血症(sUA≤6.8mg/dL)与高尿酸血症(sUA>6.8mg/dL)之间的转换率。
研究参与者的平均年龄(n = 85)为27.8±7.0岁,女性参与者占39%,非裔美国参与者占41%。sUA的平均变异系数为8.5%±4.9%(1%至23%)。男性与女性之间,以及最初为正常尿酸血症者与最初为高尿酸血症者之间的变异无显著差异。在最初为正常尿酸血症者(n = 72)中,21%在至少一次后续测量中转为高尿酸血症。与筛查sUA值在6.0 - 6.8之间的组(n = 18)相比,初始sUA<6.0的亚组(n = 54)未来出现高尿酸血症值的可能性要小得多(7%对39%,p = 0.0037)。在最初为高尿酸血症者(n = 13)中,46%在至少一次测量中后来转为正常尿酸血症。
由于自发变异,单次sUA测量在高尿酸血症分类中不可靠。了解这一点后,如果在分类中必须使用单次测量,值得注意的是,sUA<6.0mg/dL者未来出现高尿酸血症测量值的可能性较小,基于单个测量点,这可被视为排除间歇性高尿酸血症的更安全阈值。
来自母研究的数据,ClinicalTrials.gov标识符:NCT02038179 。