Department of Biomedical Engineering, McCormick School of Engineering, Northwestern University, 2145 N Sheridan Rd, Evanston, IL, 60208, USA.
Center for Bionic Medicine, Shirley Ryan AbilityLab, 355 East Erie, Chicago, IL, 60611, USA.
J Neuroeng Rehabil. 2021 Sep 8;18(1):134. doi: 10.1186/s12984-021-00924-1.
After stroke, motor control is often negatively affected, leaving survivors with less muscle strength and coordination, increased tone, and abnormal synergies (coupled joint movements) in their affected upper extremity. Humeral internal and external rotation have been included in definitions of abnormal synergy but have yet to be studied in-depth.
Determine the ability to generate internal and external rotation torque under different shoulder abduction and adduction loads in persons with chronic stroke (paretic and non-paretic arm) and uninjured controls.
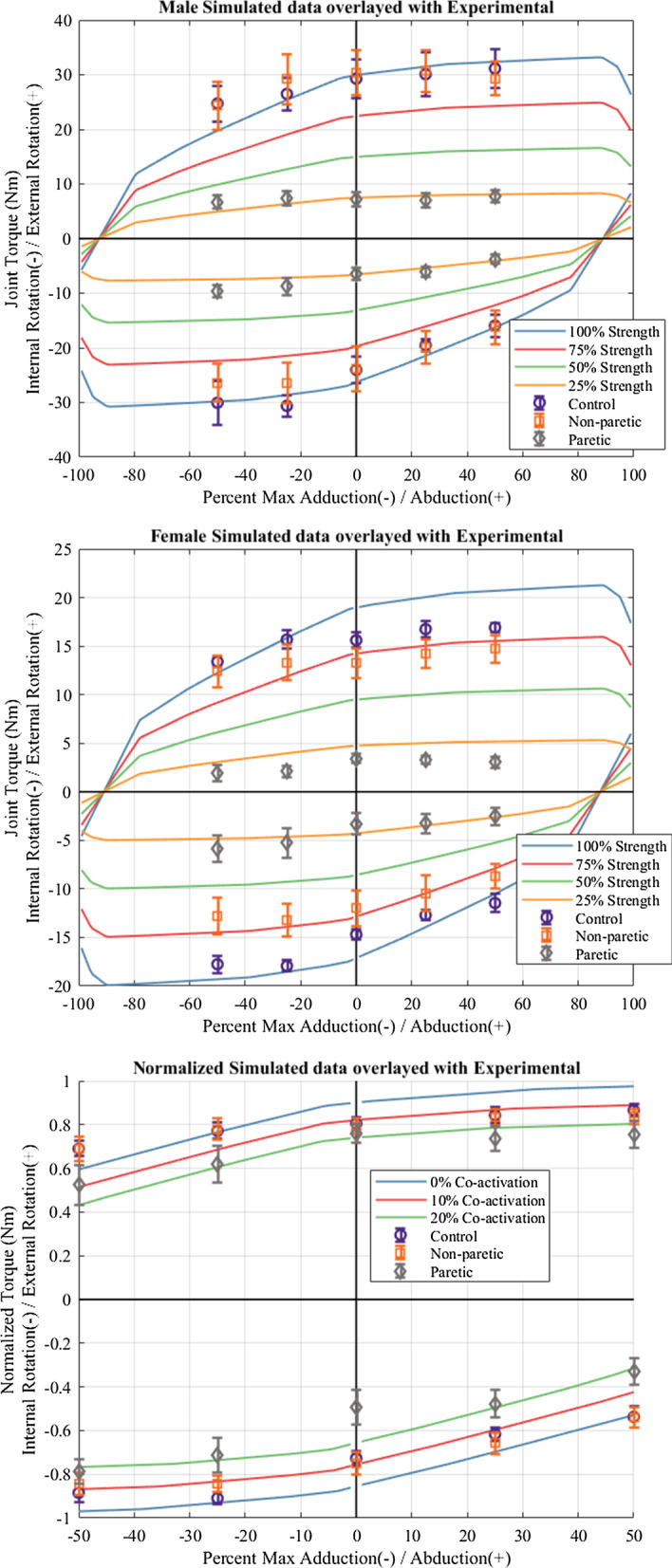
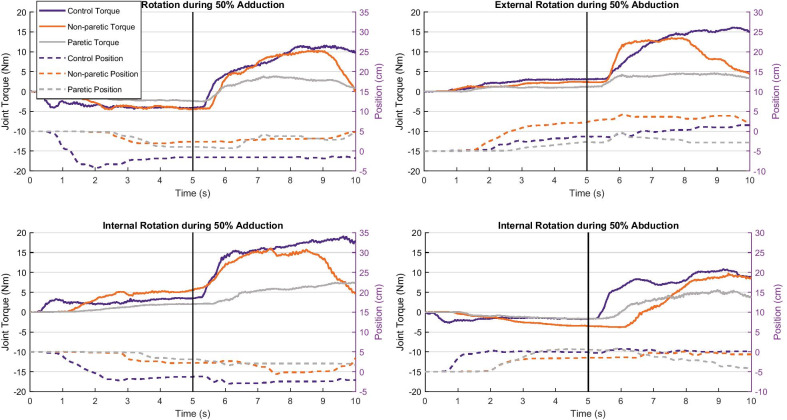
24 participants, 12 with impairments after stroke and 12 controls, completed this study. A robotic device controlled abduction and adduction loading to 0, 25, and 50% of maximum strength in each direction. Once established against the vertical load, each participant generated maximum internal and external rotation torque in a dual-task paradigm. Four linear mixed-effects models tested the effect of group (control, non-paretic, and paretic), load (0, 25, 50% adduction or abduction), and their interaction on task performance; one model was created for each combination of dual-task directions (external or internal rotation during abduction or adduction). The protocol was then modeled using OpenSim to understand and explain the role of biomechanical (muscle action) constraints on task performance.
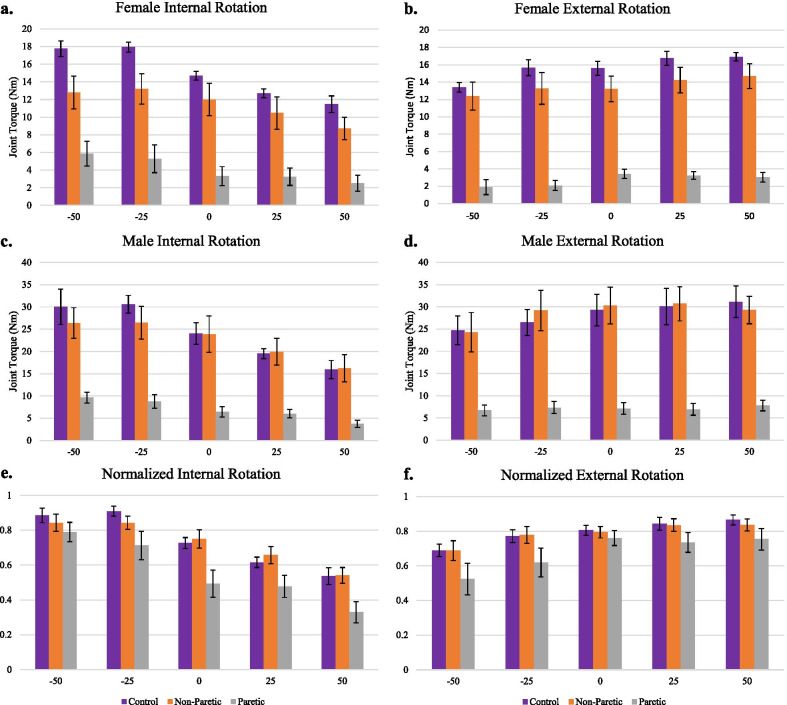
Group was significant in all task combinations. Paretic arms were less able to generate internal and external rotation during abduction and adduction, respectively. There was a significant effect of load in three of four load/task combinations for all groups. Load-level and group interactions were not significant, indicating that abduction and adduction loading affected each group in a similar manner. OpenSim musculoskeletal modeling mirrored the experimental results of control and non-paretic arms and also, when adjusted for weakness, paretic arm performance. Simulations incorporating increased co-activation mirrored the drop in performance observed across all dual-tasks in paretic arms.
Common biomechanical constraints (muscle actions) explain limitations in external and internal rotation strength during adduction and abduction dual-tasks, respectively. Additional non-load-dependent effects such as increased antagonist co-activation (hypertonia) may cause the observed decreased performance in individuals with stroke. The inclusion of external rotation in flexion synergy and of internal rotation in extension synergy may be over-simplifications.
中风后,运动控制通常会受到负面影响,使幸存者上肢肌肉力量和协调性下降、张力增加以及出现异常协同作用(关节耦合运动)。肱骨内旋和外旋已被纳入异常协同作用的定义中,但尚未进行深入研究。
确定慢性中风患者(患侧和非患侧手臂)和未受伤对照者在不同肩外展和内收负荷下产生内旋和外旋扭矩的能力。
24 名参与者完成了这项研究,其中 12 名有中风后损伤,12 名作为对照。机器人设备控制每个方向的 0、25 和 50%最大力量的外展和内收加载。在垂直负载建立后,每个参与者在双重任务范式下产生最大内旋和外旋扭矩。四个线性混合效应模型测试了组(对照、非患侧和患侧)、负荷(0、25、50%外展或内收)及其相互作用对任务表现的影响;为每个双重任务方向(外展或内收时的外旋或内旋)的组合创建了一个模型。然后使用 OpenSim 对协议进行建模,以了解和解释生物力学(肌肉活动)对任务表现的限制。
所有任务组合的组都是显著的。患侧手臂在分别进行外展和内收时,内旋和外旋的能力都较低。在所有四个负荷/任务组合中,有三个组合的负荷都有显著影响。负荷水平和组间相互作用不显著,表明外展和内收加载对所有组的影响方式相似。OpenSim 肌肉骨骼建模反映了对照和非患侧手臂的实验结果,也反映了在调整了无力的情况下患侧手臂的表现。纳入协同增加的肌肉共同激活模拟了所有双重任务中观察到的患侧手臂的性能下降。
常见的生物力学限制(肌肉活动)分别解释了在进行外展和内收双重任务时外旋和内旋力量的限制。增加拮抗剂共同激活(高张力)等非负荷依赖性影响可能导致中风患者观察到的运动表现下降。在屈肌协同作用中包括外旋以及在伸肌协同作用中包括内旋可能过于简单化。