University Health Network, University of Toronto, Toronto, Ontario, Canada
Unit of Cardiology, Karolinska Institute & Karolinska University Hospital, Stockholm, Sweden.
Clin J Am Soc Nephrol. 2021 Sep;16(9):1345-1354. doi: 10.2215/CJN.01130121. Epub 2021 Jun 18.
A reduction in the rate of eGFR decline, with preservation of ≥0.75 ml/min per 1.73 m per year, has been proposed as a surrogate for kidney disease progression. We report results from prespecified analyses assessing effects of ertugliflozin versus placebo on eGFR slope from the eValuation of ERTugliflozin effIcacy and Safety CardioVascular outcomes (VERTIS CV) trial (NCT01986881).
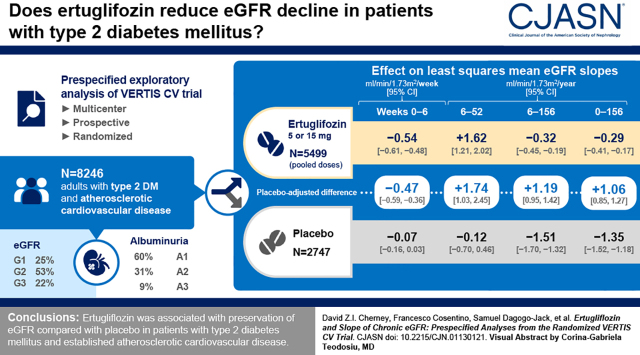
DESIGN, SETTING, PARTICIPANTS, & MEASUREMENTS: Patients with type 2 diabetes mellitus and established atherosclerotic cardiovascular disease were randomized to placebo, ertugliflozin 5 mg, and ertugliflozin 15 mg (1:1:1). The analyses compared the effect of ertugliflozin (pooled doses, =5499) versus placebo (=2747) on eGFR slope per week and per year by random coefficient models. Study periods (weeks 0-6 and weeks 6-52) and total and chronic slopes (week 0 or week 6 to weeks 104, 156, 208, and 260) were modeled separately and by baseline kidney status.
In the overall population, for weeks 0-6, the least squares mean eGFR slopes (ml/min per 1.73 m per week [95% confidence interval (95% CI)]) were -0.07 (-0.16 to 0.03) and -0.54 (-0.61 to -0.48) for the placebo and ertugliflozin groups, respectively; the difference was -0.47 (-0.59 to -0.36). During weeks 6-52, least squares mean eGFR slopes (ml/min per 1.73 m per year [95% CI]) were -0.12 (-0.70 to 0.46) and 1.62 (1.21 to 2.02) for the placebo and ertugliflozin groups, respectively; the difference was 1.74 (1.03 to 2.45). For weeks 6-156, least squares mean eGFR slopes (ml/min per 1.73 m per year [95% CI]) were -1.51 (-1.70 to -1.32) and -0.32 (-0.45 to -0.19) for the placebo and ertugliflozin groups, respectively; the difference was 1.19 (0.95 to 1.42). During weeks 0-156, the placebo-adjusted difference in least squares mean slope was 1.06 (0.85 to 1.27). These findings were consistent by baseline kidney status.
Ertugliflozin has a favorable placebo-adjusted eGFR slope >0.75 ml/min per 1.73 m per year, documenting the kidney function preservation underlying the clinical benefits of ertugliflozin on kidney disease progression in patients with type 2 diabetes mellitus and atherosclerotic cardiovascular disease.
US National Library of Medicine, ClinicalTrials.gov NCT01986881. Date of trial registration: November 13, 2013.
有人提出,eGFR 下降率的降低(保留≥0.75ml/min/1.73m/年)可作为肾脏疾病进展的替代指标。我们报告了来自预先指定的分析结果,这些分析评估了依格列净与安慰剂对 eValuation of ERTugliflozin effIcacy and Safety CardioVascular outcomes(VERTIS CV)试验(NCT01986881)中 eGFR 斜率的影响。
设计、地点、参与者和测量:将患有 2 型糖尿病和已确诊的动脉粥样硬化性心血管疾病的患者随机分配至安慰剂、依格列净 5mg 和依格列净 15mg(1:1:1)组。这些分析通过随机系数模型比较了依格列净(合并剂量,=5499)与安慰剂(=2747)对每周和每年 eGFR 斜率的影响。研究期间(第 0-6 周和第 6-52 周)以及总斜率和慢性斜率(第 0 周或第 6 周至第 104、156、208 和 260 周)分别进行了模型化,并按基线肾脏状况进行了模型化。
在总体人群中,在第 0-6 周期间,安慰剂和依格列净组的最小二乘平均 eGFR 斜率(ml/min/1.73m/周[95%置信区间(95%CI)])分别为-0.07(-0.16 至 0.03)和-0.54(-0.61 至-0.48);差异为-0.47(-0.59 至-0.36)。在第 6-52 周期间,安慰剂和依格列净组的最小二乘平均 eGFR 斜率(ml/min/1.73m/年[95%CI])分别为-0.12(-0.70 至 0.46)和 1.62(1.21 至 2.02);差异为 1.74(1.03 至 2.45)。在第 6-156 周期间,安慰剂和依格列净组的最小二乘平均 eGFR 斜率(ml/min/1.73m/年[95%CI])分别为-1.51(-1.70 至-1.32)和-0.32(-0.45 至-0.19);差异为 1.19(0.95 至 1.42)。在第 0-156 周期间,安慰剂调整后的最小二乘平均斜率差异为 1.06(0.85 至 1.27)。这些发现与基线肾脏状况一致。
依格列净具有有利的安慰剂调整后 eGFR 斜率>0.75ml/min/1.73m/年,证明了依格列净在 2 型糖尿病和动脉粥样硬化性心血管疾病患者中对肾脏疾病进展的临床获益背后存在的肾脏功能保护。
美国国立卫生研究院,ClinicalTrials.gov NCT01986881。试验注册日期:2013 年 11 月 13 日。