Klain Michele, Zampella Emilia, Piscopo Leandra, Volpe Fabio, Manganelli Mariarosaria, Masone Stefania, Pace Leonardo, Salvatore Domenico, Schlumberger Martin, Cuocolo Alberto
Department of Advanced Biomedical Sciences, University Federico II, 80131 Naples, Italy.
Department of Clinical Medicine and Surgery, University Federico II, 80131 Naples, Italy.
Cancers (Basel). 2021 Aug 27;13(17):4338. doi: 10.3390/cancers13174338.
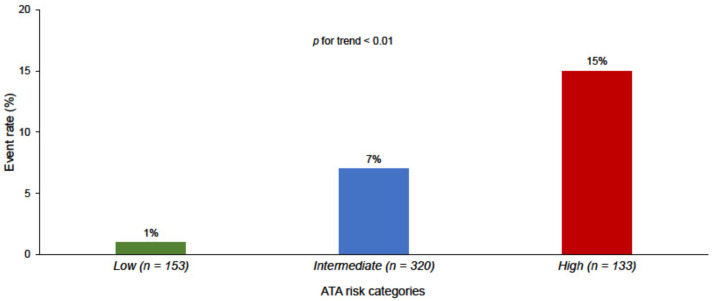
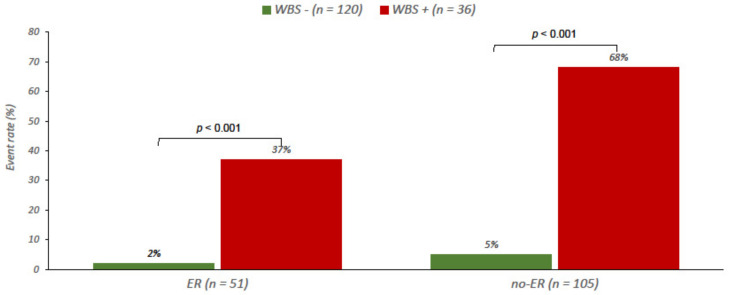
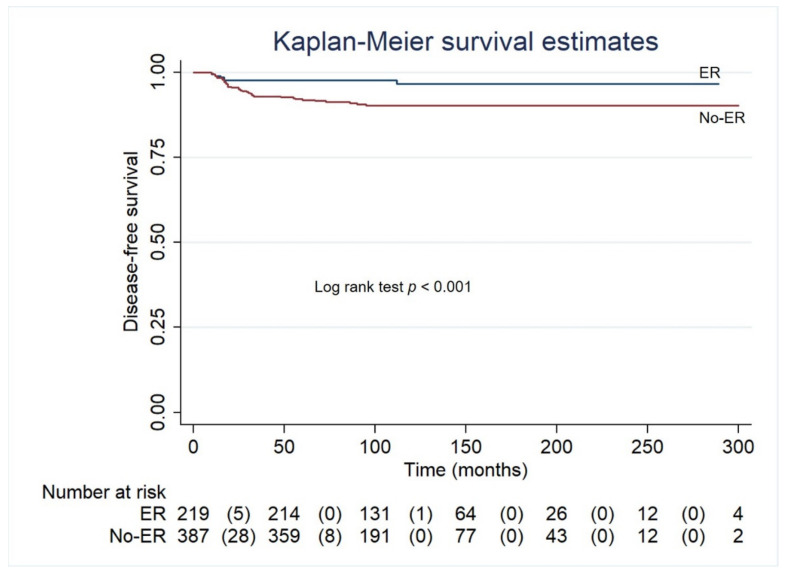
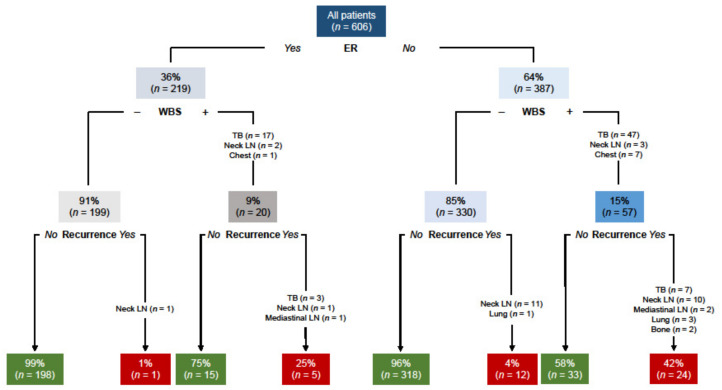
This study assessed the long-term predictive value of the response to therapy, evaluated by serum thyroglobulin (Tg) determination and neck ultrasound, and estimated the potential additional impact of diagnostic whole-body scan (WBS) in patients with differentiated thyroid cancer (DTC) treated with surgery and radioactive iodine (RAI) therapy. We retrospectively evaluated 606 DTC patients treated with surgery and RAI. Response to I therapy at 12 months was assessed by serum Tg measurement, neck ultrasound, and diagnostic WBS. According to American Thyroid Association (ATA) guidelines, patients were classified as having a low, intermediate or high risk of recurrence and at 12 months as having an excellent response (ER) or no-ER. Follow-up was then performed every 6-12 months with serum Tg determination and imaging procedures. With a median follow-up of 105 months (range 10-384), 42 (7%) events requiring further treatments occurred. Twenty-five patients had additional RAI therapy, 11 with structural disease in the thyroid bed, eight in both thyroid bed and neck lymph nodes, four had lung metastases and two had bone metastases. The other 17 patients had additional surgery for nodal disease followed by RAI therapy. The ATA intermediate and high risk of recurrence, post-operative and pre-RAI therapy Tg ≥ 10 ng/mL, and the absence of ER at 12 months were independent predictors of events. Diagnostic WBS at 12 months permitted the identification of only five recurrences among the 219 ER patients according to serum Tg levels and ultrasound. In DTC patients, the response to therapy at 12 months after RAI therapy could rely on serum Tg measurement and neck ultrasound, while diagnostic WBS was not routinely indicated in patients considered in ER.
本研究评估了通过血清甲状腺球蛋白(Tg)测定和颈部超声评估的治疗反应的长期预测价值,并估计了诊断性全身扫描(WBS)对接受手术和放射性碘(RAI)治疗的分化型甲状腺癌(DTC)患者的潜在额外影响。我们回顾性评估了606例接受手术和RAI治疗的DTC患者。通过血清Tg测量、颈部超声和诊断性WBS评估12个月时对碘治疗的反应。根据美国甲状腺协会(ATA)指南,患者被分类为具有低、中或高复发风险,在12个月时被分类为具有良好反应(ER)或无ER。然后每6 - 12个月进行随访,测定血清Tg并进行影像学检查。中位随访时间为105个月(范围10 - 384个月),发生了42例(7%)需要进一步治疗的事件。25例患者接受了额外的RAI治疗,其中11例甲状腺床有结构性病变,8例甲状腺床和颈部淋巴结均有病变,4例有肺转移,2例有骨转移。另外17例患者因淋巴结疾病接受了额外手术,随后接受RAI治疗。ATA复发风险为中、高,术后和RAI治疗前Tg≥10 ng/mL,以及12个月时无ER是事件的独立预测因素。根据血清Tg水平和超声,12个月时的诊断性WBS仅在219例ER患者中识别出5例复发。在DTC患者中,RAI治疗后12个月的治疗反应可依赖血清Tg测量和颈部超声,而在被认为有ER的患者中,诊断性WBS并非常规必需。