Center for Prevention of Cardiovascular Disease, Section on Cardiovascular Medicine, Department of Internal Medicine, Wake Forest University Baptist Medical Center, Winston-Salem, North Carolina, USA.
The Department of Biostatistics and Data Sciences, Wake Forest University School of Medicine, Winston-Salem, North Carolina, USA.
J Am Coll Cardiol. 2021 Sep 14;78(11):1083-1094. doi: 10.1016/j.jacc.2021.07.016.
Little is known about the relationship between lipoprotein (a) [Lp(a)] and high-sensitivity C-reactive protein (hsCRP) and their joint association with atherosclerotic cardiovascular disease (ASCVD).
The purpose of this study was to assess whether Lp(a)-associated ASCVD risk is modified by hsCRP in the context of primary prevention.
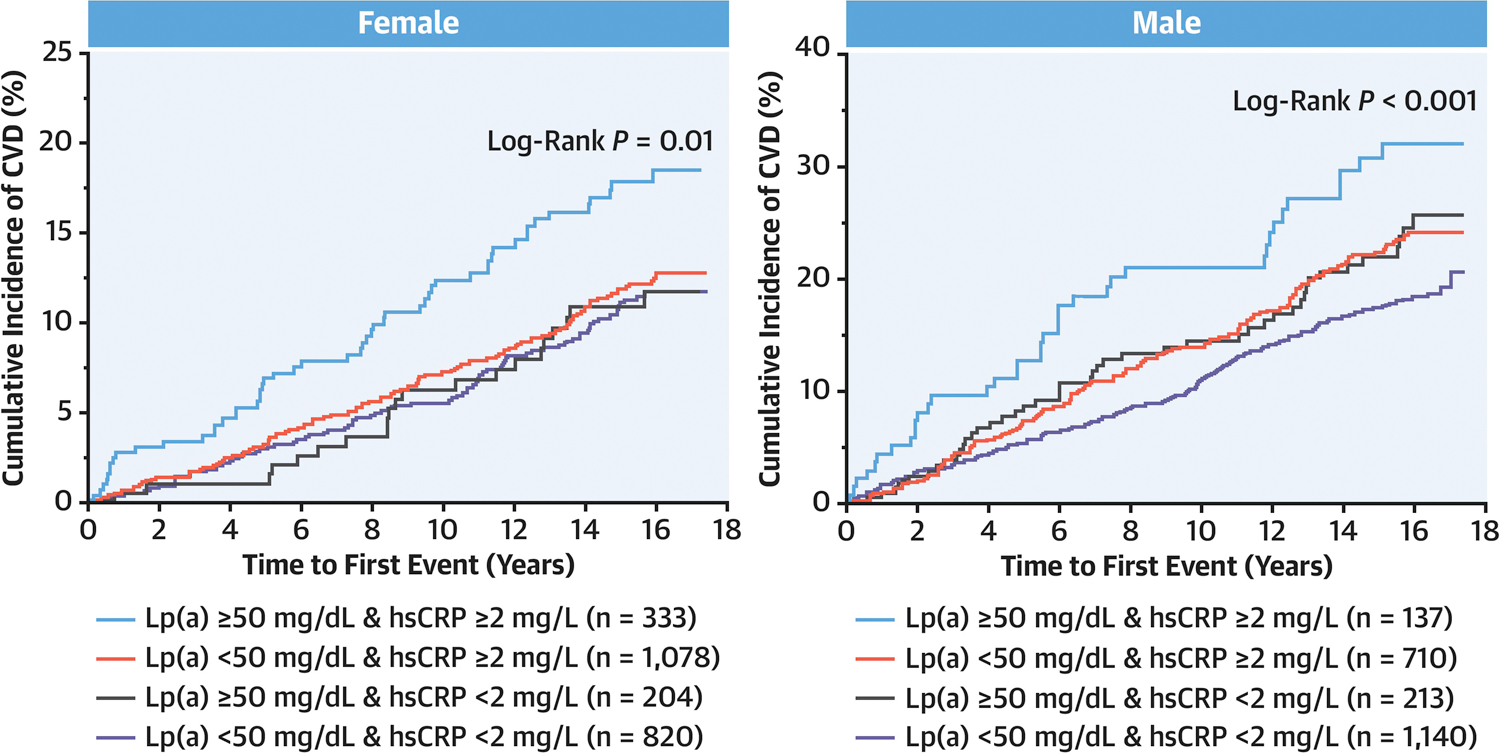
The current study included 4,679 participants from the MESA (Multi-Ethnic Study of Atherosclerosis) Apolipoprotein ancillary data set. Cox proportional hazards models and Kaplan-Meier curves were used to assess the association among Lp(a), hsCRP, and time to cardiovascular disease (CVD) events.
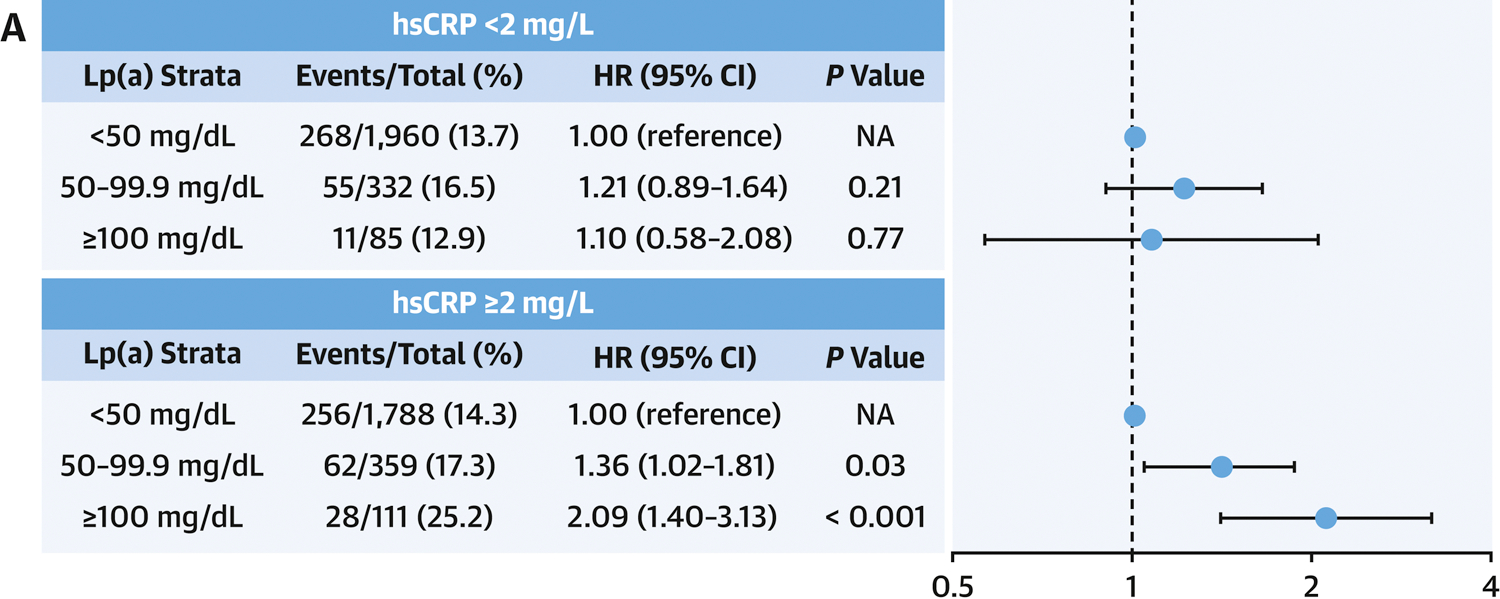
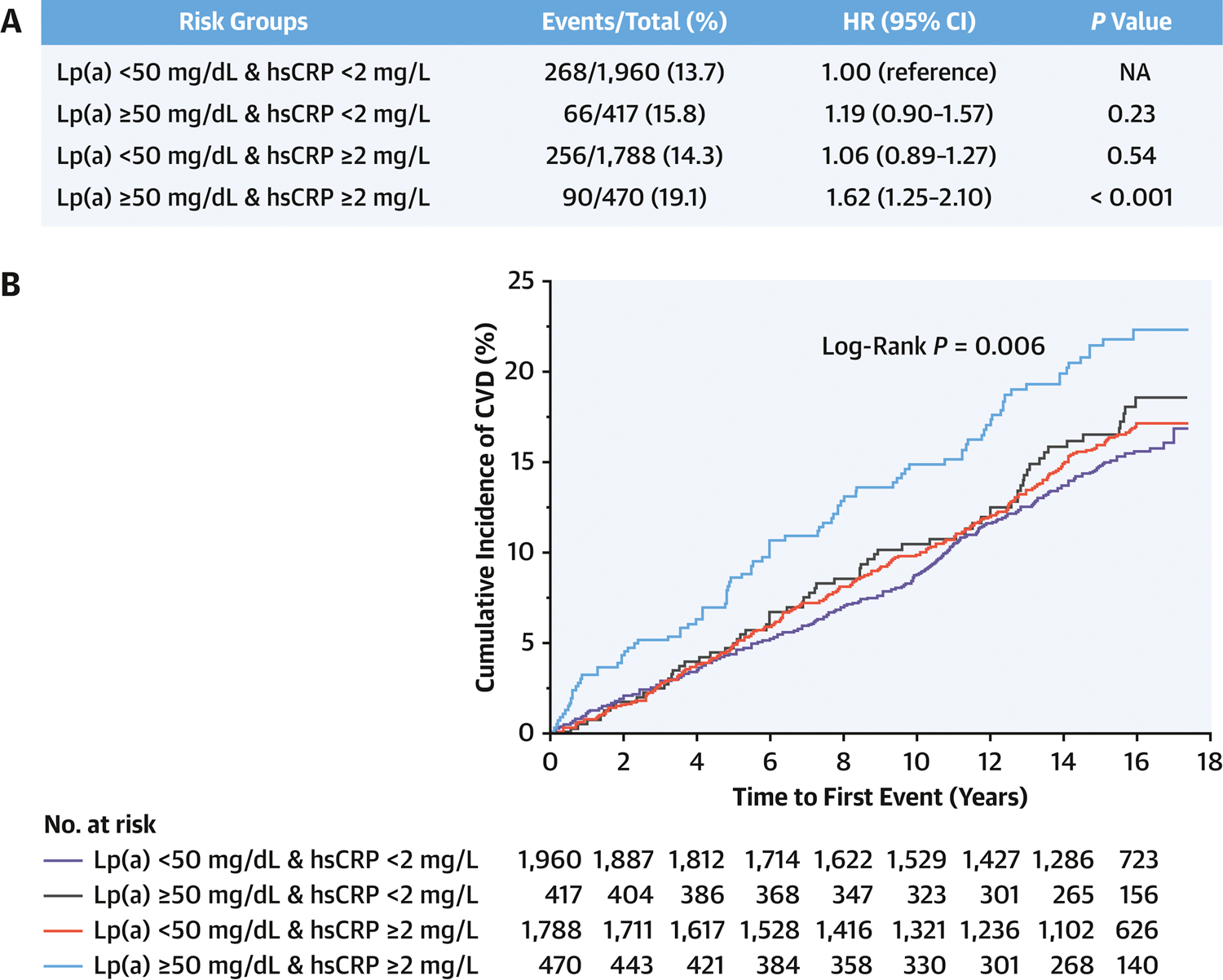
During a mean follow-up of 13.6 years, 684 CVD events occurred. A significant interaction was observed between Lp(a) and hsCRP (P = 0.04). With hsCRP <2 mg/L, no significant CVD risk was observed at any level of Lp(a) from <50 mg/dL to >100 mg/dL. However, with hsCRP ≥2 mg/L, a significant CVD risk was observed with Lp(a) of 50-99.9 mg/dL (HR: 1.36; 95% CI: 1.02-1.81) and Lp(a) ≥100 mg/dL (HR: 2.09; 95% CI: 1.40-3.13). Isolated elevations of either Lp(a) or hsCRP were not associated with increased CVD risk. In contrast, the combination of elevated Lp(a) (≥50 mg/dL) and hsCRP (≥2 mg/L) was independently associated with significant CVD risk (HR: 1.62; 95% CI: 1.25-2.10) and all-cause mortality (HR: 1.39; 95% CI: 1.12-1.72).
Lp(a)-associated ASCVD risk is observed only with concomitant elevation of hsCRP. Individuals with concomitant presence of elevated Lp(a) and systemic inflammation have greater ASCVD risk and all-cause mortality, and thus may merit closer surveillance and more aggressive ASCVD risk management.
脂蛋白(a)[Lp(a)]与高敏 C 反应蛋白(hsCRP)之间的关系及其与动脉粥样硬化性心血管疾病(ASCVD)的联合相关性知之甚少。
本研究旨在评估在一级预防中,Lp(a)相关的 ASCVD 风险是否受 hsCRP 的影响。
本研究纳入了 MESA(动脉粥样硬化多民族研究)载脂蛋白辅助数据集的 4679 名参与者。使用 Cox 比例风险模型和 Kaplan-Meier 曲线评估 Lp(a)、hsCRP 与心血管疾病(CVD)事件发生时间之间的相关性。
在平均 13.6 年的随访期间,发生了 684 例 CVD 事件。观察到 Lp(a)与 hsCRP 之间存在显著的交互作用(P=0.04)。当 hsCRP<2mg/L 时,Lp(a)水平从<50mg/dL 至>100mg/dL 之间,无论在任何水平均未观察到明显的 CVD 风险。然而,当 hsCRP≥2mg/L 时,Lp(a)为 50-99.9mg/dL(HR:1.36;95%CI:1.02-1.81)和 Lp(a)≥100mg/dL(HR:2.09;95%CI:1.40-3.13)时,观察到明显的 CVD 风险。单独升高 Lp(a)或 hsCRP 与 CVD 风险增加无关。相反,升高的 Lp(a)(≥50mg/dL)和 hsCRP(≥2mg/L)的组合与显著的 CVD 风险(HR:1.62;95%CI:1.25-2.10)和全因死亡率(HR:1.39;95%CI:1.12-1.72)独立相关。
仅在 hsCRP 同时升高时才观察到 Lp(a)相关的 ASCVD 风险。同时存在升高的 Lp(a)和全身炎症的个体具有更高的 ASCVD 风险和全因死亡率,因此可能需要更密切的监测和更积极的 ASCVD 风险管理。