Division of Endocrinology, Department of Medicine, Cumming School of Medicine, 1820 Richmond Rd SW, Calgary, AB, T2T 5C7, Canada.
Department of Endocrinology, University Hospitals Birmingham NHS Foundation Trust, Birmingham, UK.
Sci Rep. 2021 Sep 9;11(1):17947. doi: 10.1038/s41598-021-97247-x.
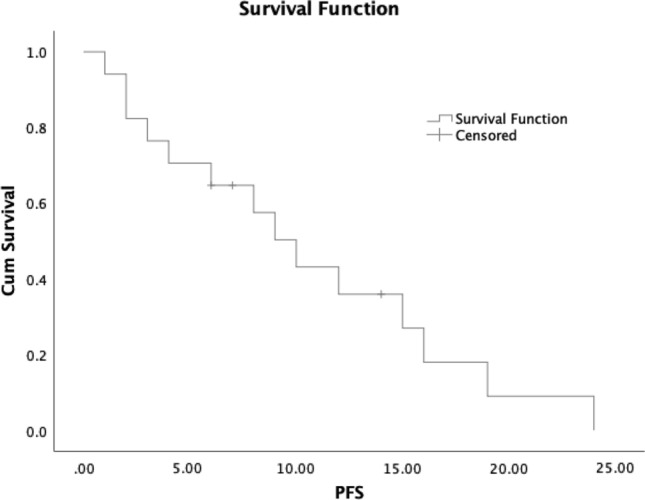
Neuroendocrine neoplasms are known to have heterogeneous biological behavior. G3 neuroendocrine tumours (NET G3) are characterized by well-differentiated morphology and Ki67 > 20%. The prognosis of this disease is understood to be intermediate between NET G2 and neuroendocrine carcinoma (NEC). Clinical management of NET G3 is challenging due to limited data to inform treatment strategies. We describe clinical characteristics, treatment, and outcomes in a large single centre cohort of patients with gastroenteropancreatic NET G3. Data was reviewed from 26 cases managed at Queen Elizabeth Hospital, Birmingham, UK, from 2012 to 2019. Most commonly the site of the primary tumour was unknown and majority of cases with identifiable primaries originated in the GI tract. Majority of cases demonstrated somatostatin receptor avidity. Median Ki67 was 30%, and most cases had stage IV disease at diagnosis. Treatment options included surgery, somatostatin analogs (SSA), and chemotherapy with either platinum-based or temozolomide-based regimens. Estimated progression free survival was 4 months following initiation of SSA and 3 months following initiation of chemotherapy. Disease control was observed following treatment in 5/11 patients treated with chemotherapy. Estimated median survival was 19 months; estimated 1 year survival was 60% and estimated 2 year survival was 13%. NET G3 is a heterogeneous group of tumours and patients which commonly have advanced disease at presentation. Prognosis is typically poor, though select cases may respond to treatment with SSA and/or chemotherapy. Further study is needed to compare efficacy of different treatment strategies for this disease.
神经内分泌肿瘤的生物学行为具有异质性。G3 神经内分泌肿瘤(NET G3)的特点是分化良好的形态学和 Ki67>20%。这种疾病的预后被认为介于 NET G2 和神经内分泌癌(NEC)之间。由于缺乏治疗策略的相关数据,NET G3 的临床管理具有挑战性。我们描述了英国伯明翰伊丽莎白女王医院 2012 年至 2019 年间收治的 26 例胃肠胰神经内分泌肿瘤 G3 患者的临床特征、治疗方法和结局。大多数情况下,原发肿瘤的部位未知,大多数可识别原发肿瘤的病例起源于胃肠道。大多数病例显示出生长抑素受体亲和力。中位数 Ki67 为 30%,大多数病例在诊断时已处于 IV 期疾病。治疗选择包括手术、生长抑素类似物(SSA)和化疗,包括铂类或替莫唑胺为基础的方案。SSA 起始后无进展生存估计为 4 个月,化疗起始后无进展生存估计为 3 个月。11 例接受化疗的患者中有 5 例在治疗后观察到疾病得到控制。估计中位生存时间为 19 个月;估计 1 年生存率为 60%,估计 2 年生存率为 13%。NET G3 是一组异质性肿瘤和患者,通常在就诊时就已处于晚期疾病状态。预后通常较差,但某些病例可能对 SSA 和/或化疗治疗有反应。需要进一步研究以比较这种疾病的不同治疗策略的疗效。