Department of Pediatric Immunology and Rheumatology, Wilhelmina Children's Hospital, Utrecht, The Netherlands.
Clinica Pediatrica e Reumatologia, IRCCS Istituto Giannina Gaslini.
Rheumatology (Oxford). 2022 May 5;61(5):2104-2112. doi: 10.1093/rheumatology/keab678.
To describe risk factors for IBD development in a cohort of children with JIA.
JIA patients who developed IBD were identified from the international Pharmachild register. Characteristics were compared between IBD and non-IBD patients and predictors of IBD were determined using multivariable logistic regression analysis. Incidence rates of IBD events on different DMARDs were calculated, and differences between therapies were expressed as relative risks (RR).
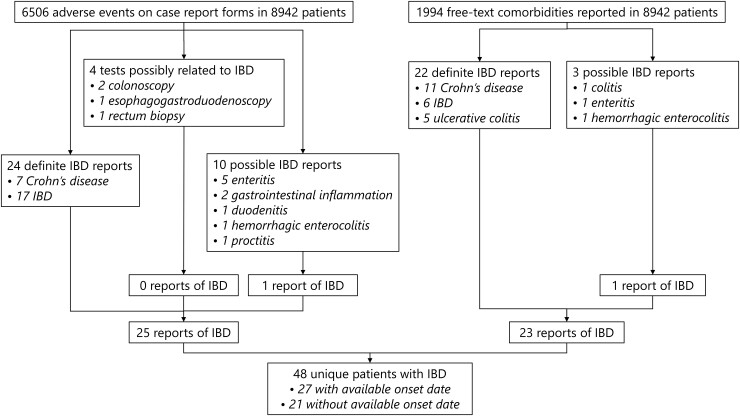
Out of 8942 patients, 48 (0.54% ) developed IBD. These were more often male (47.9% vs 32.0%) and HLA-B27 positive (38.2% vs 21.0%) and older at JIA onset (median 8.94 vs 5.33 years) than patients without IBD development. They also had more often a family history of autoimmune disease (42.6% vs 24.4%) and enthesitis-related arthritis (39.6% vs 10.8%). The strongest predictors of IBD on multivariable analysis were enthesitis-related arthritis [odds ratio (OR): 3.68, 95% CI: 1.41, 9.40] and a family history of autoimmune disease (OR: 2.27, 95% CI: 1.12, 4.54). Compared with methotrexate monotherapy, the incidence of IBD on etanercept monotherapy (RR: 7.69, 95% CI: 1.99, 29.74), etanercept with methotrexate (RR: 5.70, 95% CI: 1.42, 22.77) and infliximab (RR: 7.61, 95% CI: 1.27, 45.57) therapy was significantly higher. Incidence on adalimumab was not significantly different (RR: 1.45, 95% CI: 0.15, 13.89).
IBD in JIA was associated with enthesitis-related arthritis and a family history of autoimmune disease. An increased IBD incidence was observed for etanercept therapy regardless of concomitant methotrexate use.
描述幼年特发性关节炎(JIA)患儿队列中炎症性肠病(IBD)发展的危险因素。
从国际 Pharmachild 登记处确定发生 IBD 的 JIA 患者。比较 IBD 患者与非 IBD 患者的特征,并使用多变量逻辑回归分析确定 IBD 的预测因素。计算不同 DMARD 上 IBD 事件的发生率,并通过相对风险(RR)表示治疗之间的差异。
在 8942 名患者中,有 48 名(0.54%)发生 IBD。这些患者更常见于男性(47.9%比 32.0%)和 HLA-B27 阳性(38.2%比 21.0%),且发病时年龄更大(中位数 8.94 岁比 5.33 岁)。与未发生 IBD 发展的患者相比,他们也更常患有自身免疫性疾病家族史(42.6%比 24.4%)和附着点相关关节炎(39.6%比 10.8%)。多变量分析中 IBD 的最强预测因素是附着点相关关节炎[比值比(OR):3.68,95%置信区间(CI):1.41,9.40]和自身免疫性疾病家族史(OR:2.27,95% CI:1.12,4.54)。与甲氨蝶呤单药治疗相比,依那西普单药治疗(RR:7.69,95% CI:1.99,29.74)、依那西普联合甲氨蝶呤(RR:5.70,95% CI:1.42,22.77)和英夫利昔单抗(RR:7.61,95% CI:1.27,45.57)治疗的 IBD 发生率显著更高。阿达木单抗的发生率无显著差异(RR:1.45,95% CI:0.15,13.89)。
JIA 中的 IBD 与附着点相关关节炎和自身免疫性疾病家族史有关。无论是否同时使用甲氨蝶呤,依那西普治疗均可观察到 IBD 发病率增加。