British Columbia Centre for Disease Control, Vancouver, BC, Canada.
School of Population and Public Health, University of British Columbia (UBC), Vancouver, BC, Canada.
BMC Womens Health. 2021 Sep 13;21(1):330. doi: 10.1186/s12905-021-01470-7.
Women living with hepatitis C virus (HCV) are rarely addressed in research and may be overrepresented within key populations requiring additional support to access HCV care and treatment. We constructed the HCV care cascade among people diagnosed with HCV in British Columbia, Canada, as of 2019 to compare progress in care and treatment and to assess sex/gender gaps in HCV treatment access.
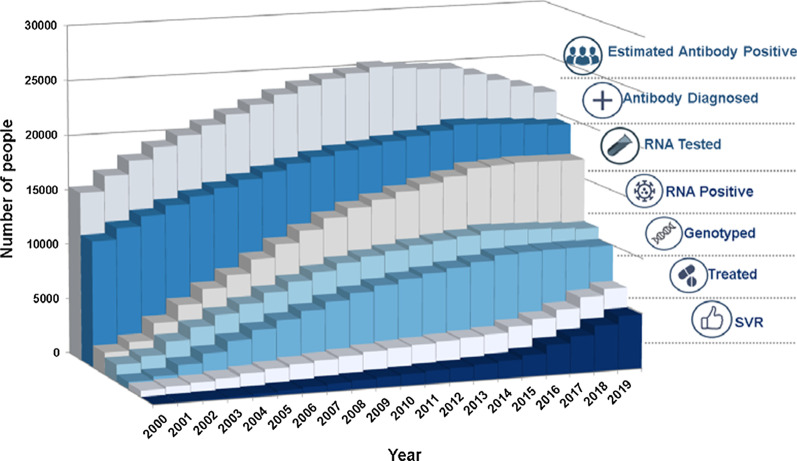
The BC Hepatitis Testers Cohort includes 1.7 million people who tested for HCV, HIV, reported cases of hepatitis B, and active tuberculosis in BC from 2000 to 2019. Test results were linked to medical visits, hospitalizations, cancers, prescription drugs, and mortality data. Six HCV care cascade stages were identified: (1) antibody diagnosed; (2) RNA tested; (3) RNA positive; (4) genotyped; (5) initiated treatment; and (6) achieved sustained virologic response (SVR). HCV care cascade results were assessed for women, and an 'inverse' cascade was created to assess gaps, including not being RNA tested, genotyped, or treatment initiated, stratified by sex.
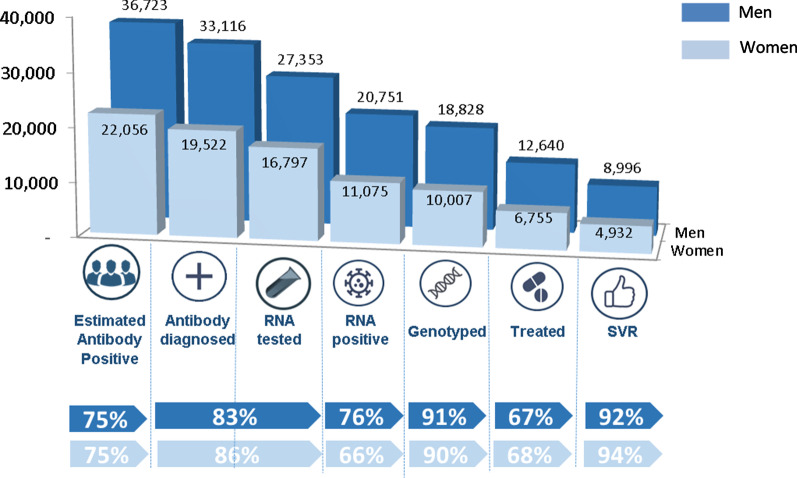
In 2019, 52,638 people with known sex were anti-HCV positive in BC; 37% (19,522) were women. Confirmatory RNA tests were received by 86% (16,797/19,522) of anti-HCV positive women and 83% (27,353/33,116) of men. Among people who had been genotyped, 68% (6756/10,008) of women and 67% (12,640/18,828) of men initiated treatment, with 94% (5023/5364) of women and 92% (9147/9897) of men achieving SVR. Among the 3252 women and 6188 men not yet treated, higher proportions of women compared to men were born after 1975 (30% vs. 21%), had a mental health diagnosis (42% vs. 34%) and had used injection drugs (50% vs. 45%). Among 1619 women and 2780 men who had used injection drugs and were not yet treated, higher proportions of women than men used stimulants (64% vs. 57%), and opiates (67% vs. 60%).
Women and men appear to be equally engaged into the HCV care cascade; however, women with concurrent social and health conditions are being left behind. Treatment access may be improved with approaches that meet the needs of younger women, those with mental health diagnoses, and women who use drugs.
在研究中,很少关注患有丙型肝炎病毒 (HCV) 的女性,而在需要额外支持以获得 HCV 护理和治疗的重点人群中,她们可能占比过高。我们构建了截至 2019 年在不列颠哥伦比亚省 (BC) 诊断为 HCV 的人群的 HCV 护理级联,以比较护理和治疗方面的进展,并评估 HCV 治疗机会的性别差距。
BC 肝炎检测者队列包括 2000 年至 2019 年期间在 BC 进行 HCV、HIV 检测、报告乙型肝炎病例和活动性肺结核的 170 万人。检测结果与医疗就诊、住院、癌症、处方药和死亡率数据相关联。确定了六个 HCV 护理级联阶段:(1) 抗体诊断;(2) RNA 检测;(3) RNA 阳性;(4) 基因分型;(5) 开始治疗;和 (6) 实现持续病毒学应答 (SVR)。对女性进行了 HCV 护理级联结果评估,并创建了一个“反转”级联,以评估差距,包括未进行 RNA 检测、基因分型或治疗开始,按性别分层。
2019 年,BC 有已知性别的 52,638 人抗 HCV 阳性;其中 37%(19,522 人)为女性。86%(16,797/19,522)的抗 HCV 阳性女性和 83%(27,353/33,116)的男性接受了确认性 RNA 检测。在已进行基因分型的人群中,68%(6756/10,008)的女性和 67%(12,640/18,828)的男性开始治疗,其中 94%(5023/5364)的女性和 92%(9147/9897)的男性达到 SVR。在未接受治疗的 3252 名女性和 6188 名男性中,与男性相比,出生于 1975 年后的女性比例更高(30%比 21%),有心理健康诊断的女性比例更高(42%比 34%),使用过注射毒品的女性比例更高(50%比 45%)。在已使用注射毒品且未接受治疗的 1619 名女性和 2780 名男性中,使用兴奋剂的女性比例高于男性(64%比 57%),使用阿片类药物的女性比例高于男性(67%比 60%)。
女性和男性似乎都同样参与了 HCV 护理级联;然而,同时患有社会和健康状况的女性却被抛在了后面。通过满足年轻女性、有心理健康诊断的女性和使用毒品的女性的需求,治疗机会可能会得到改善。