Department of Hepatology, Toranomon Hospital, Japan.
Okinaka Memorial Institute for Medical Research, Toranomon Hospital, Japan.
Intern Med. 2022 Apr 1;61(7):951-958. doi: 10.2169/internalmedicine.7589-21. Epub 2021 Sep 11.
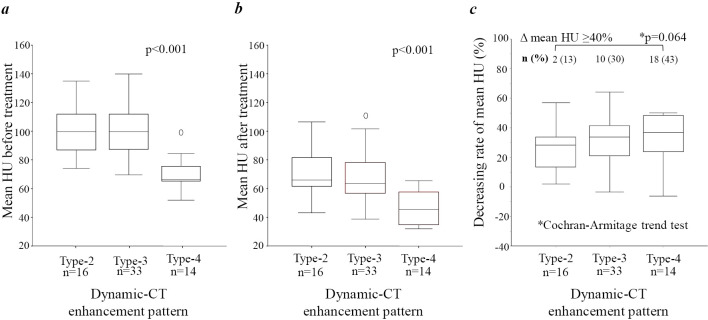
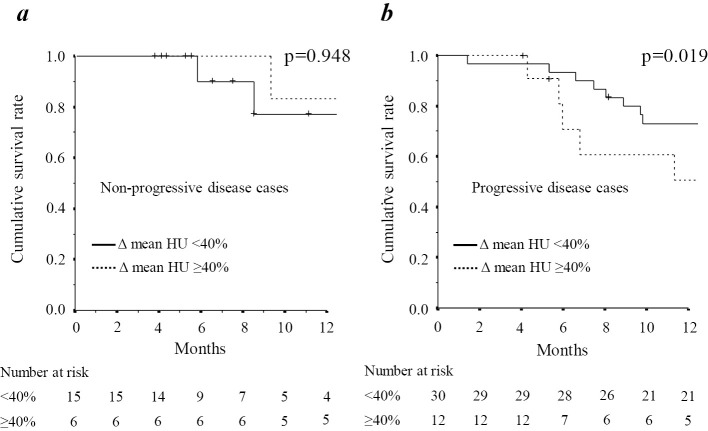
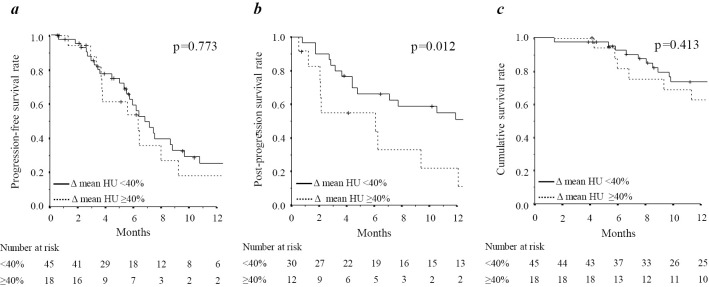
Objective The relationship between the prognosis and magnitude of a decrease in tumor blood flow according to estimated tumor differentiation remains unclear. This study investigated the relationship between reductions in the rate of mean computed tomography (CT) attenuation values and the clinical prognosis. Methods We evaluated 63 consecutive patients who received lenvatinib treatment for unresectable hepatocellular carcinoma (HCC). The oncological aggressiveness of the tumors was estimated using classification by dynamic CT enhancement patterns. The utility of changes in mean CT attenuation values of intra-hepatic targets during treatment to estimate the prognosis was investigated by calculating the progression-free survival (PFS) and post-progression survival (PPS). A multivariate analysis was used to identify potential confounders for the survival after progression during lenvatinib therapy. Results The rate of decrease in the mean CT attenuation value gradually increased according to the degree of deterioration in estimated tumor differentiation, and the rate of a decrease in attenuation ≥40% showed a tendency to increase (p=0.064). This trend was reflected by a better objective response in oncological aggressiveness heterogeneous enhancement patterns (Type-3 and Type-4) than a homogeneous enhancement pattern (Type-2) (83% vs. 56% of modified Response Evaluation Criteria in Solid Tumors). This resulted in a similar PFS between the groups (p=0.773), whereas the PPS was significantly worse when the rate of decrease in the attenuation value was ≥40% (p=0.012). A multivariate analysis confirmed that a rate of decease in attenuation value ≥40% was a poor prognostic factor for the PPS (hazard ratio, 2.993; 95% confidence interval, 1.196-7.490; p=0.019). Conclusion A rate of decrease in attenuation ≥40% may reflect a good response of a highly malignant tumor to lenvatinib. Therefore, this value may have utility as a surrogate marker for estimating the oncological aggressiveness of tumors and their associated prognosis.
目的 根据肿瘤分化程度的估计,肿瘤血流减少的预后和幅度之间的关系尚不清楚。本研究调查了平均 CT(计算机断层扫描)衰减值降低率与临床预后之间的关系。
方法 我们评估了 63 例连续接受仑伐替尼治疗不可切除肝细胞癌(HCC)的患者。使用基于动态 CT 增强模式的分类来评估肿瘤的肿瘤侵袭性。通过计算无进展生存期(PFS)和进展后生存期(PPS),研究了治疗过程中肝内靶标平均 CT 衰减值变化对预后的估计作用。使用多变量分析来确定仑伐替尼治疗期间进展后生存的潜在混杂因素。
结果 平均 CT 衰减值的降低率根据肿瘤分化程度的恶化程度逐渐增加,并且衰减率降低≥40%的趋势增加(p=0.064)。这种趋势反映在肿瘤侵袭性异质性增强模式(类型 3 和类型 4)的客观反应比均质性增强模式(类型 2)更好(83%比 56%的改良实体瘤反应评估标准)。这导致两组之间的 PFS 相似(p=0.773),而当衰减值的降低率≥40%时,PPS 明显更差(p=0.012)。多变量分析证实,衰减值降低率≥40%是 PPS 的不良预后因素(危险比,2.993;95%置信区间,1.196-7.490;p=0.019)。
结论 衰减率降低≥40%可能反映了高度恶性肿瘤对仑伐替尼的良好反应。因此,该值可作为估计肿瘤侵袭性及其相关预后的替代标志物。